
Lumbar Spine Anatomy Anatomical Foundation
Detailed exploration of lumbar spine anatomy, disc structure, neural elements, and biomechanical function. Understanding normal lumbar anatomy is essential for appreciating how disc replacement surgery restores optimal function and eliminates chronic back pain.
Lumbar Support
Structural Framework
5 Vertebrae
Five lumbar vertebrae (L1-L5) providing major structural support for the upper body while maintaining flexibility for daily activities and movement.
Nerve Pathways
Critical Networks
Complex
Complex nerve pathways including the cauda equina and nerve roots requiring precise anatomical understanding for safe surgical intervention.
Load Distribution
Function Analysis
Biomechanical
Sophisticated biomechanical load distribution systems allowing complex movements while maintaining stability and protecting neural structures.
Lumbar Spine ArchitectureL1 to L5 (and S1)
The lumbar spine is the workhorse of human back, sitting between the thoracic spine above and the sacrum/pelvis below. Where the cervical spine prioritises mobility, the lumbar spine prioritises load-bearing and power transfer.
Motion Segments for Disc Replacement
These levels are where most degenerative disc disease and mechanical back pain arise.
Clinical Relevance for Disc Replacement
Endplate strength and bone quality are critical for implant anchorage. Osteoporosis or very poor bone quality may contraindicate disc replacement or require modified strategy.
Facet Joints & StabilityMotion Guides and Load Sharers
Each lumbar motion segment has one intervertebral disc anteriorly and two facet joints posteriorly — together forming the critical “three-joint complex”.
Facet Joint Anatomy
True synovial joints with specialised structures:
Biomechanical Role
- Limit shear (sliding) between vertebrae
- Restrict excessive rotation
- Guide flexion/extension movements
- Provide sensory input via richly innervated capsules
Facet Joint Degeneration Cascade
Stage 1: Cartilage Wear
Initial cartilage breakdown and joint space narrowing
Disc Replacement Context: Lumbar disc replacement assumes relatively preserved facet joints. Advanced facet arthrosis is a red flag and may shift surgical choice toward fusion rather than arthroplasty.
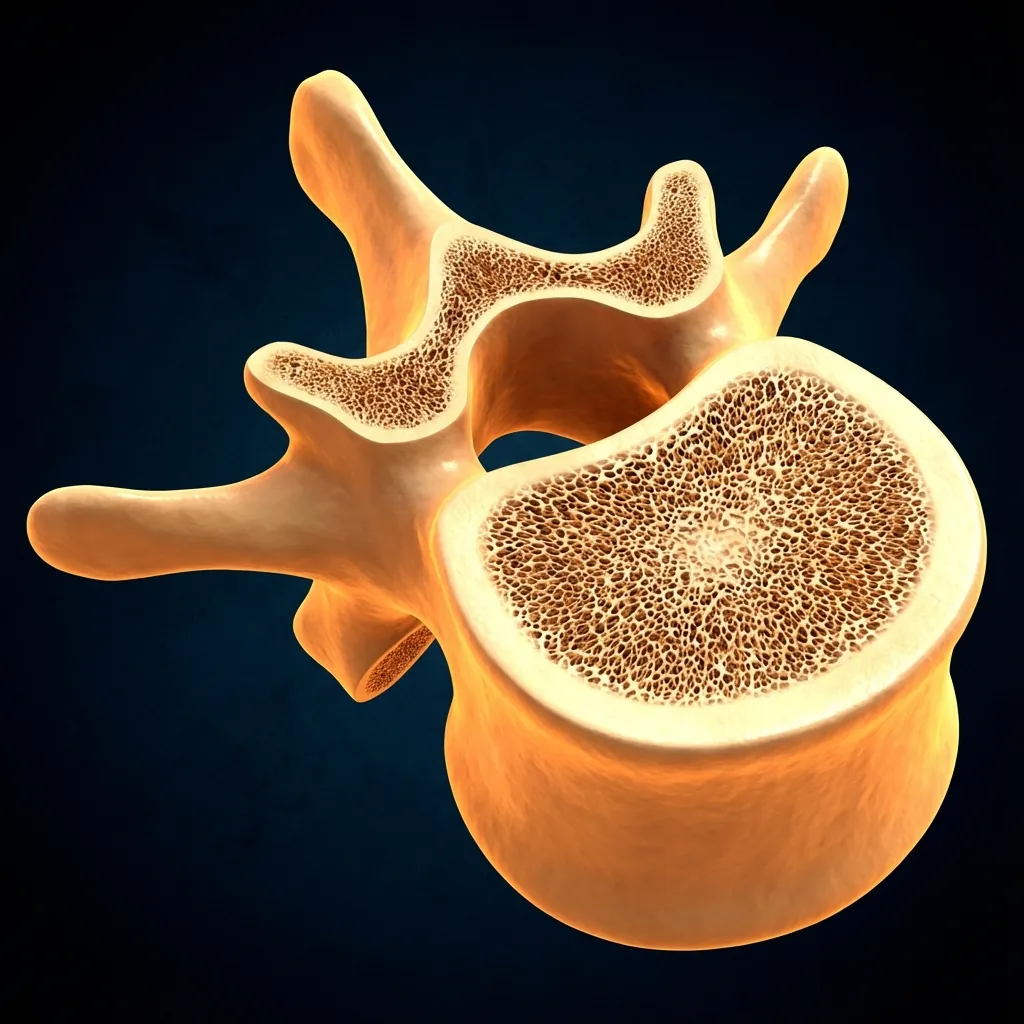
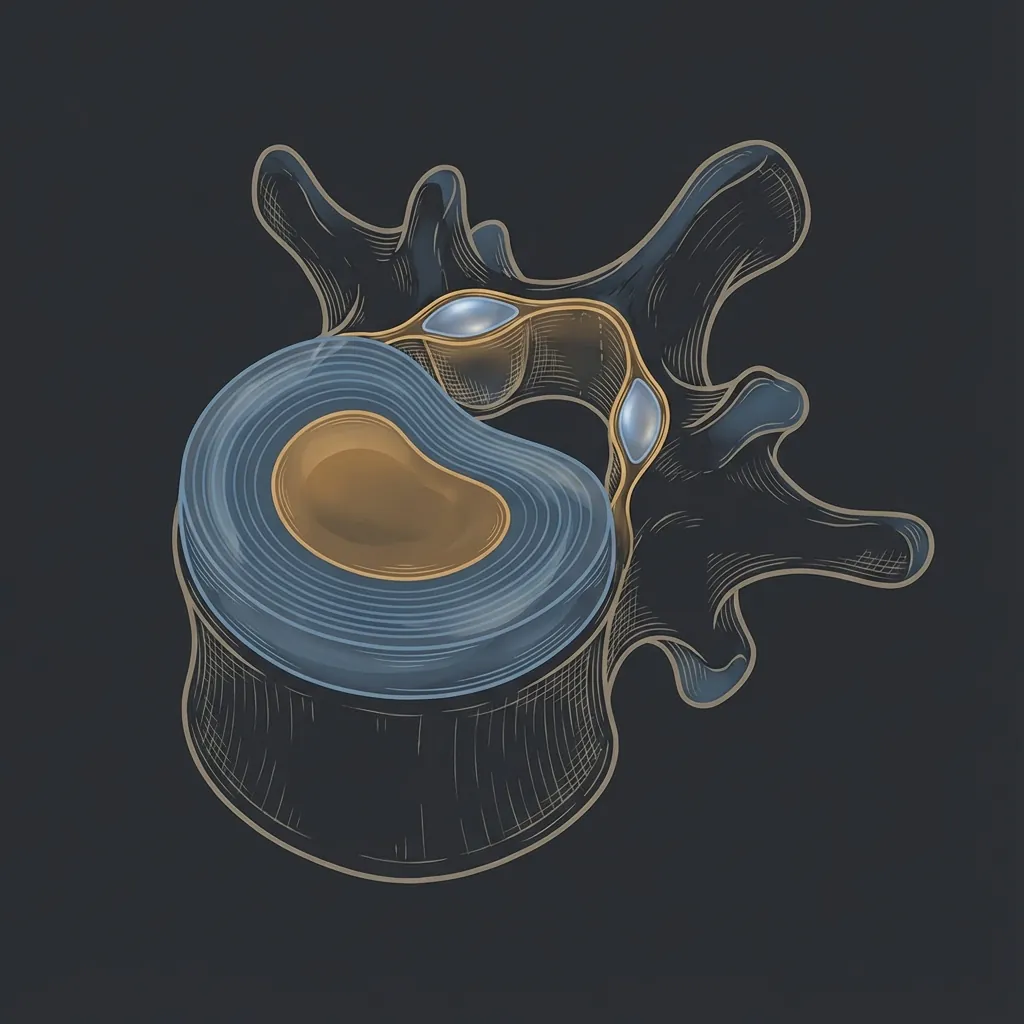
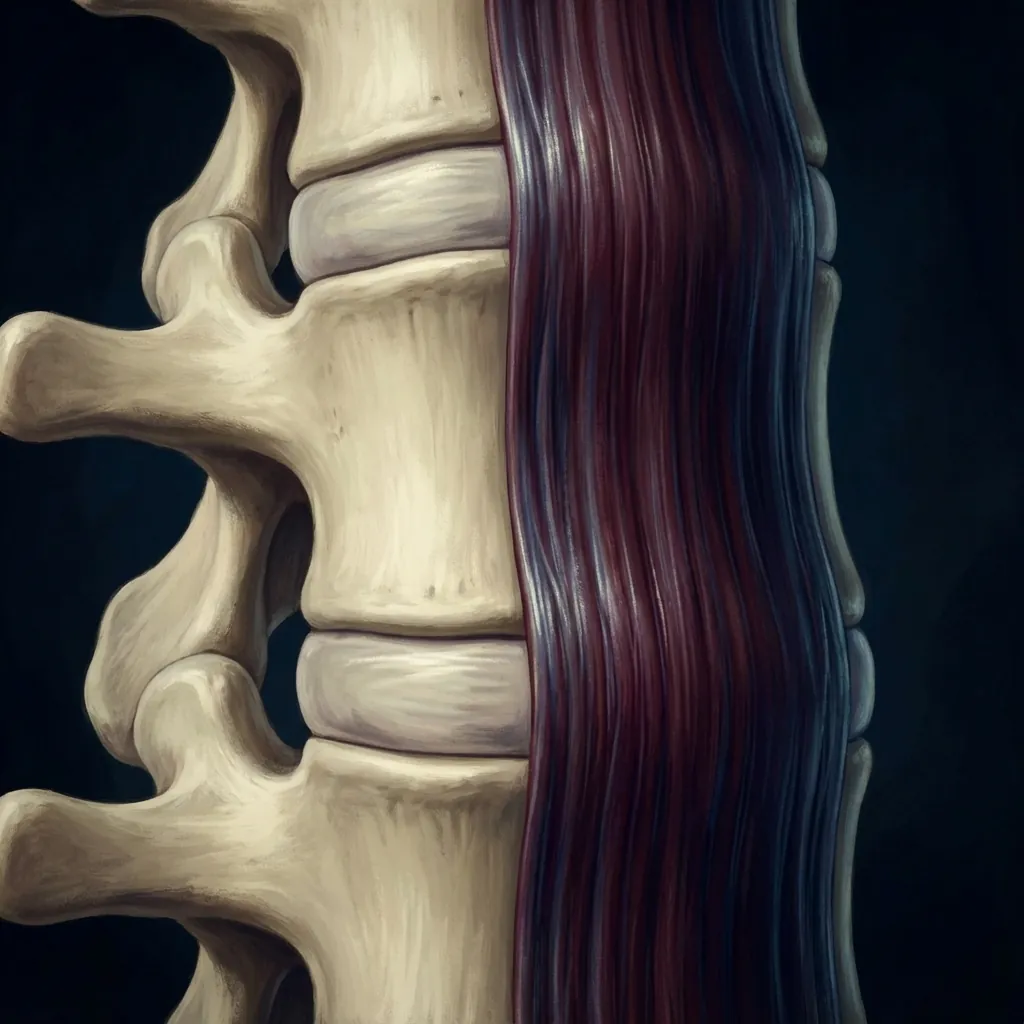
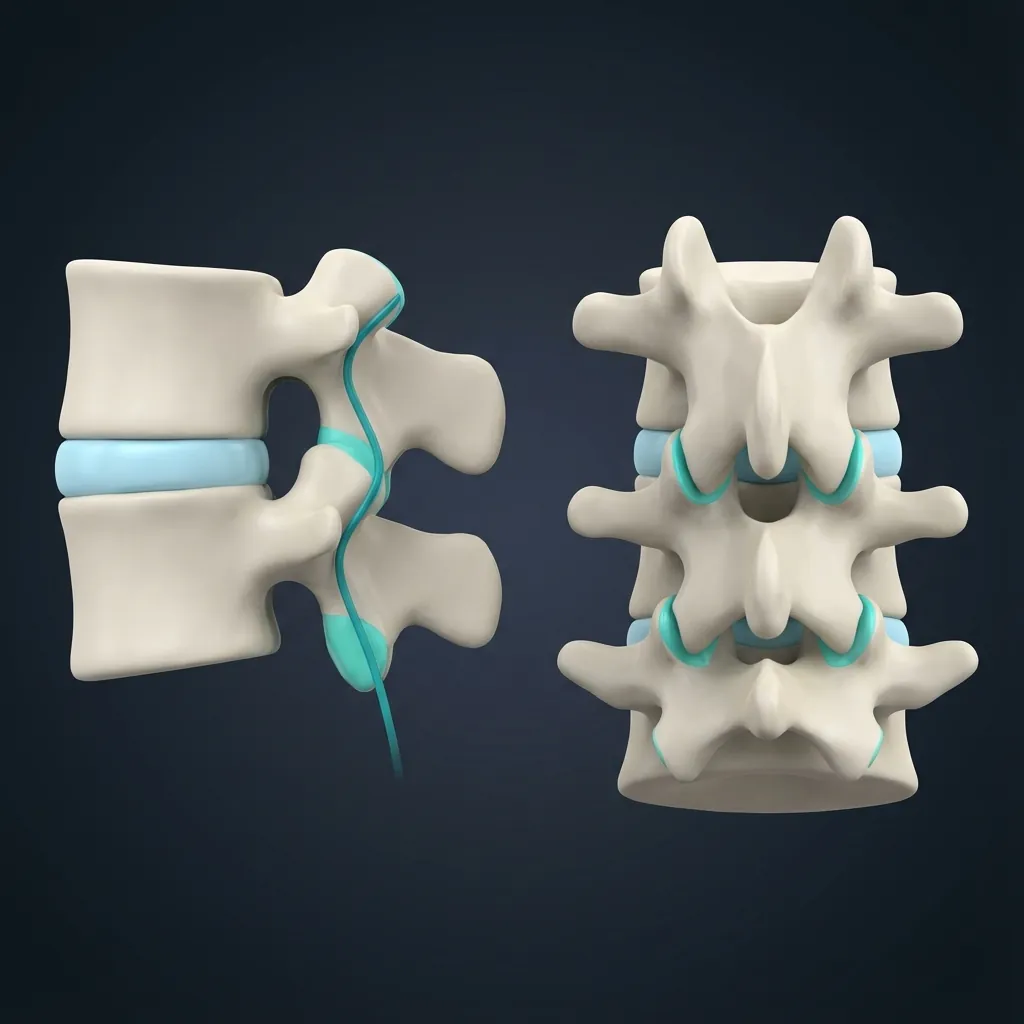
Lumbar Disc StructureLoad Spreaders and Motion Couplers
Between each pair of lumbar vertebrae lies an intervertebral disc. These discs transmit and distribute compressive loads, allow controlled motion, and maintain spacing for nerve roots to exit safely.
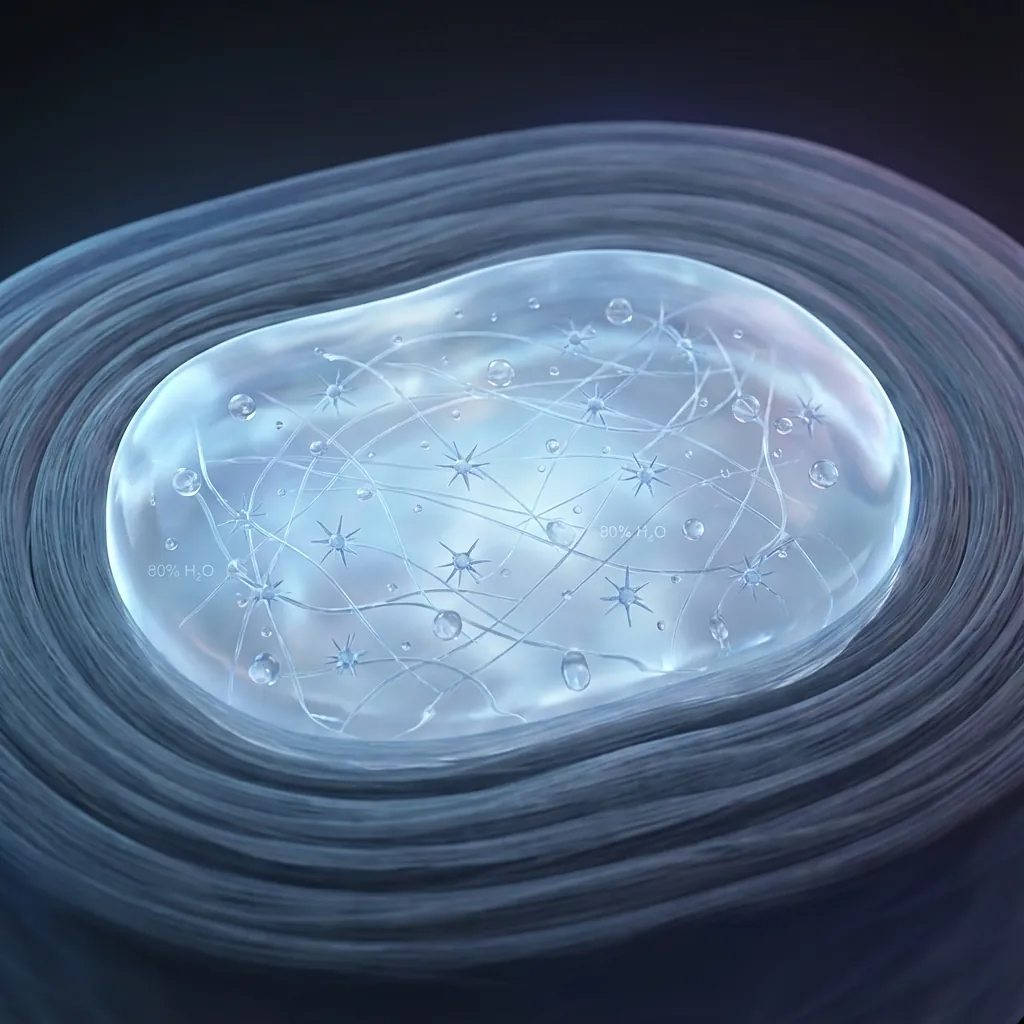
Nucleus Pulposus
Central gel-like core
Composition
~70–90% water in healthy young adult
Rich in proteoglycans (e.g., aggrecan) that bind water
Contains type II collagen and specialised disc cells
Function
Behaves like a pressurised fluid under load
Distributes forces evenly across endplates
Maintains disc height (and therefore foraminal height)
Age-Related Changes
• Proteoglycan content declines
• Water content decreases (desiccation)
• Nucleus becomes more fibrous, less gel-like
• Load-sharing capacity declines
Disc Replacement Consideration
During disc replacement, endplates must be prepared carefully to seat the implant without compromising structural strength. The goal is optimal implant anchorage while preserving the nutrient pathway function.
Neural ElementsFrom Cord to Cauda Equina
Unlike the cervical region, the spinal cord usually ends around L1 as the conus medullaris. Below this level, the canal contains the cauda equina — a bundle of lumbar and sacral nerve roots.
Cervical Pathology
Can compress spinal cord → Myelopathy
Lumbar Pathology
Usually compresses nerve roots → Radiculopathy or Cauda Equina Syndrome
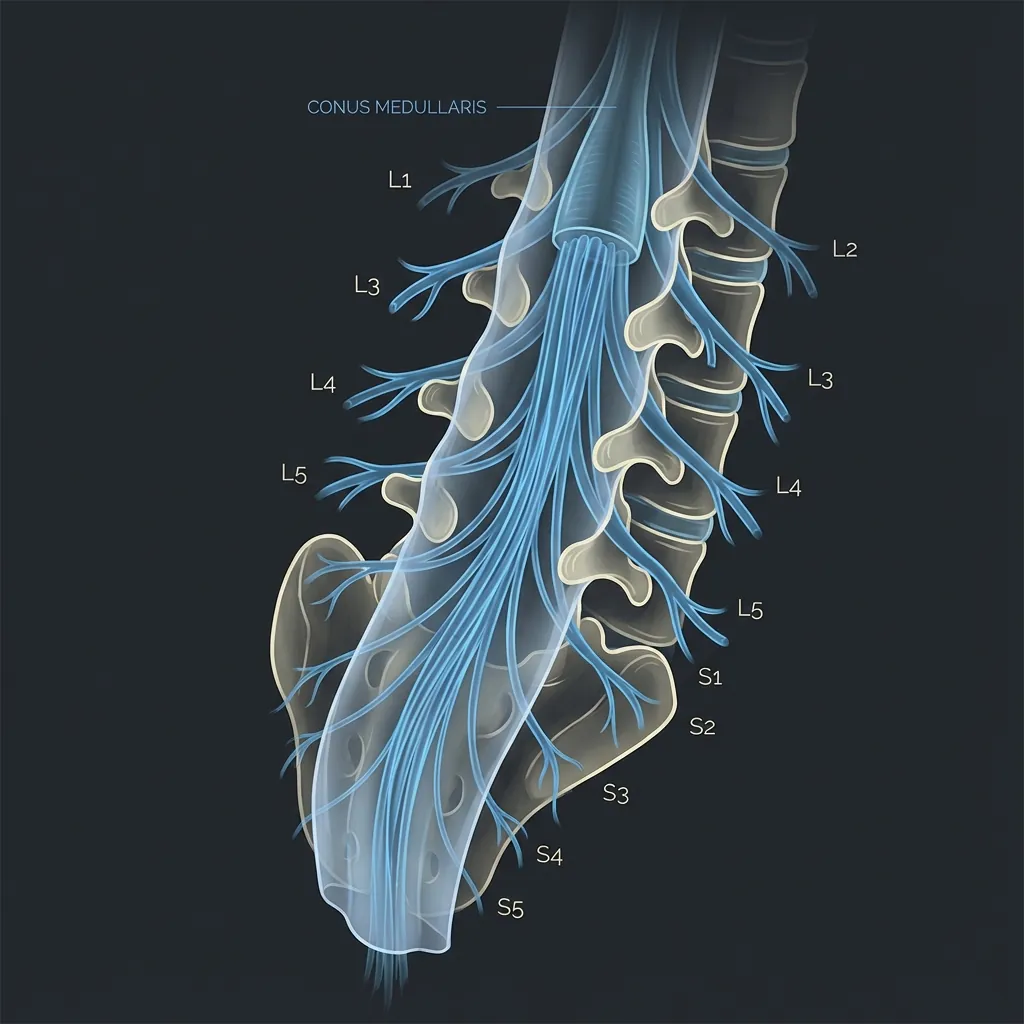
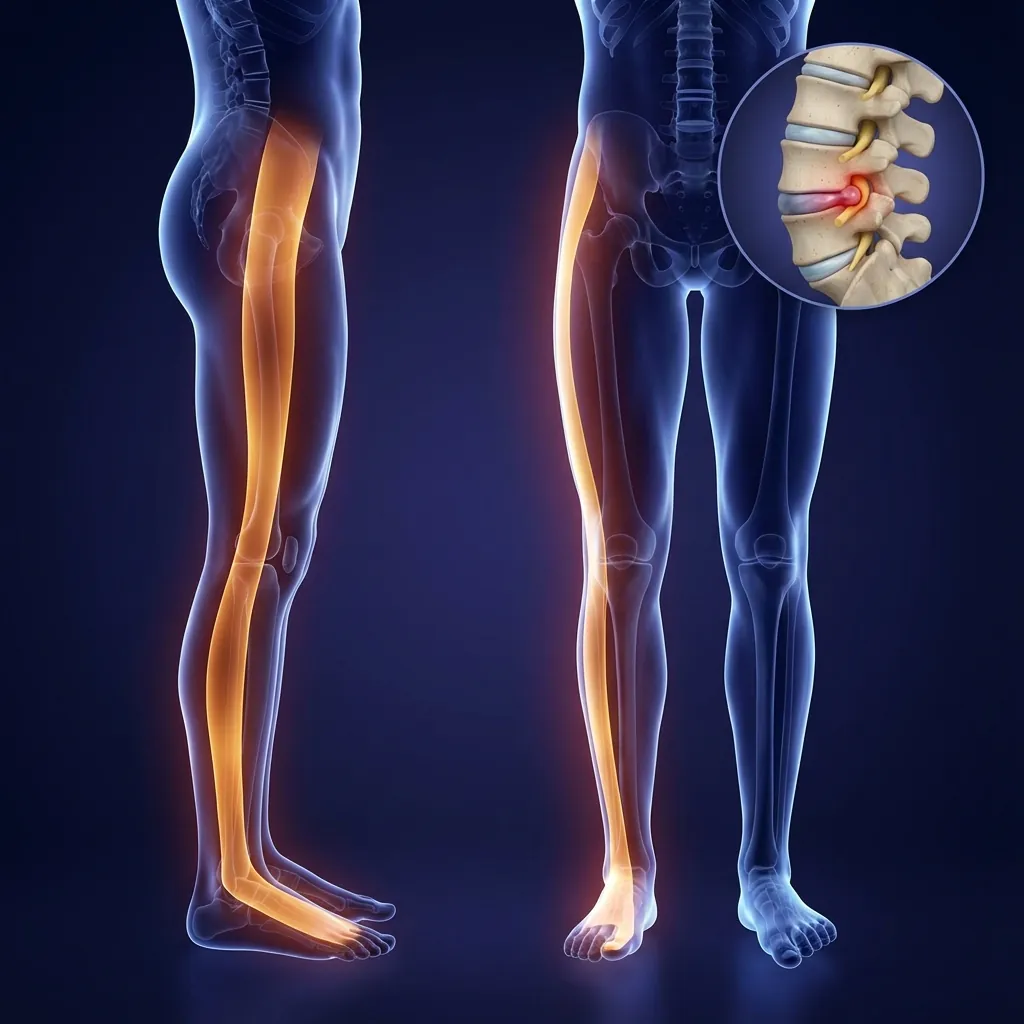
Lumbar Nerve Roots and Dermatomes
Radiculopathy Patterns
- Anterior thigh/knee pain
- Reduced knee jerk
- Quadriceps weakness
- Difficulty climbing stairs, rising from squat
- Lateral leg and dorsum foot pain
- Big toe weakness
- Foot drop or tripping over toes
- Usually normal reflexes
- Posterior leg pain, calf involvement
- Lateral foot numbness
- Weakened plantarflexion
- Reduced Achilles reflex
Intervertebral Foramen
Each lumbar nerve root exits through a foramen bordered by:
Foraminal Narrowing Causes
- Disc bulge or herniation
- Posterior osteophytes
- Facet joint hypertrophy/arthrosis
- Spondylolisthesis (vertebral slip)
Even small encroachment can be significant when combined with inflammation and swelling.
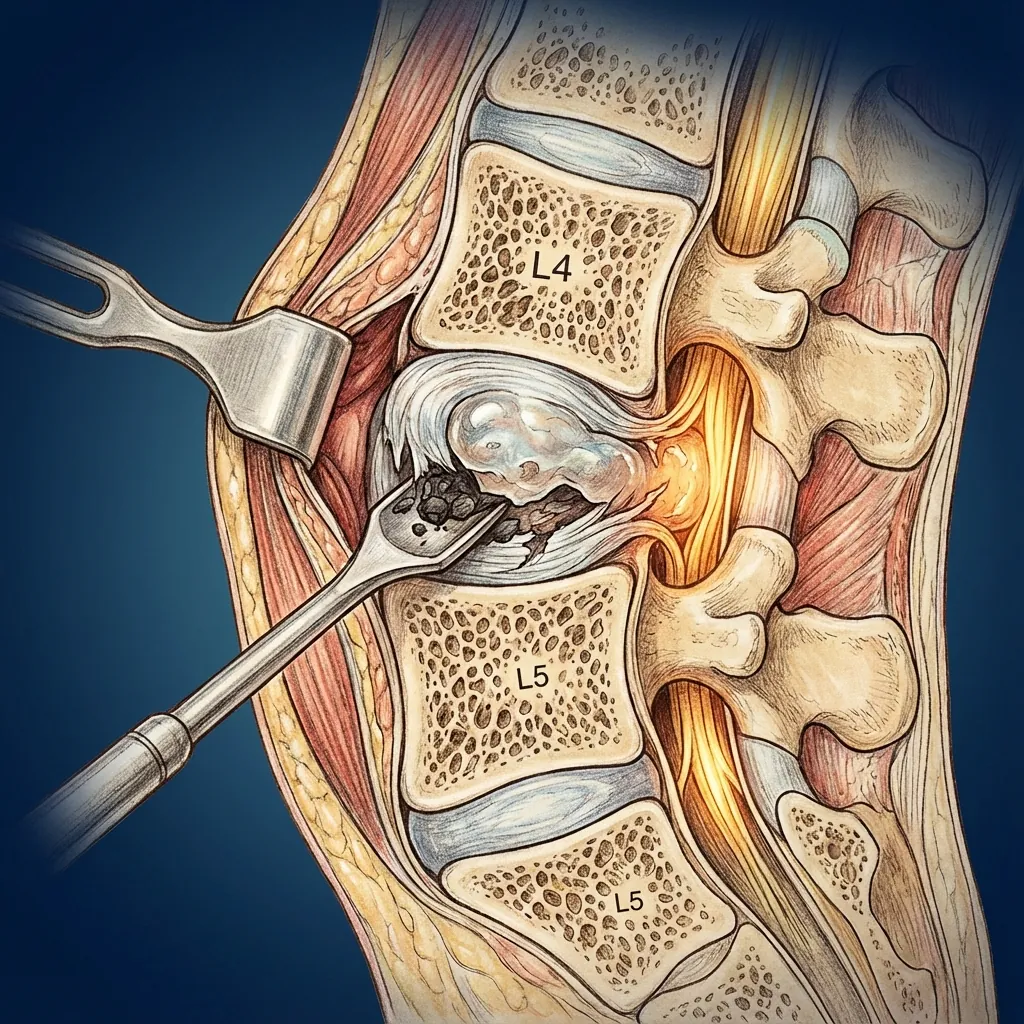
Cauda Equina Syndrome (Red Flag)
Severe central lumbar disc herniation (usually at L4–5 or L5–S1) can compress multiple cauda equina nerve roots, causing:
This is a SURGICAL EMERGENCY. Decompression should occur as soon as possible to reduce risk of permanent neurological deficit.
Relevance for Disc Replacement
The symptom pattern plus imaging identifies which disc is responsible. Successful disc replacement requires decompression of the relevant nerve root and restoration of foraminal height.
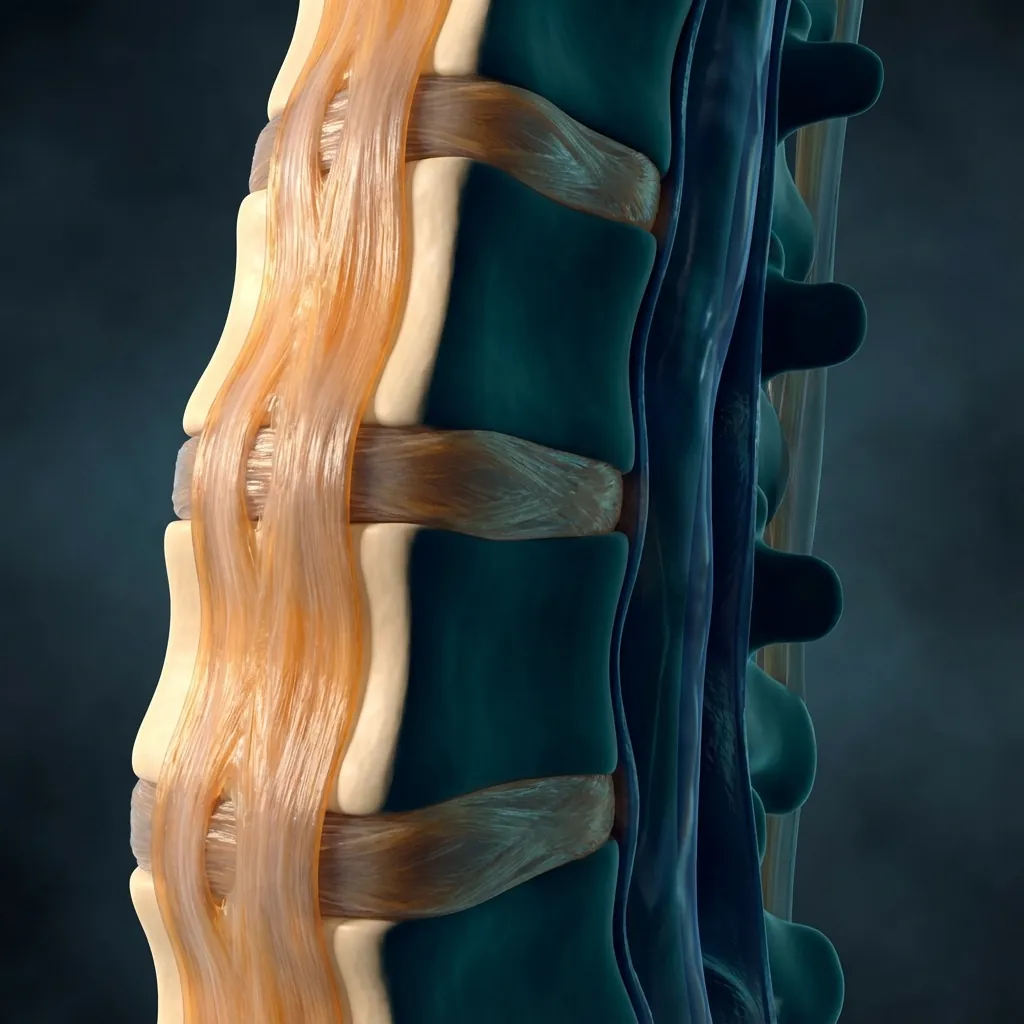
Ligamentous SupportThe Stabilising Network
The lumbar spine is stabilised by a robust ligamentous network that works in concert with muscles and bones to maintain spinal integrity during movement and loading.



Ligament Degeneration & Stenosis
Over time, ligamentous changes contribute significantly to spinal stenosis:
Elasticity Loss
Ligaments lose their natural elasticity over time
Hypertrophy
Thickening occurs, especially in ligamentum flavum
Buckling
Ligaments fold inward during extension
Stenosis
Combined with disc bulge and facet overgrowth, narrows canal and foramina
Disc Replacement Consideration: In disc replacement candidates, severe multi-level stenosis or marked ligament/facet degeneration may limit suitability for motion-preserving surgery.
Lumbar BiomechanicsWhy the Lumbar Spine is Prone to Degeneration
The lumbar spine carries the majority of trunk weight, transmits ground reaction forces during walking, running, and lifting, and experiences significant bending and torsional loads — particularly at L4–L5 and L5–S1.
PSI peak pressure during heavy lifting
Junction between mobile spine and fixed pelvis
Global lumbar flexion range
Motion Ranges
Load Sharing: Disc vs Facets
Repeated or sustained extension in a degenerative spine can be painful due to increased facet loading.

Intra-Disc Pressures (Relative)
Lying flat
Baseline reference
Standing bent
Poor posture
Poor technique
Clinical Takeaway
Chronic poor posture and repeated high-load bending place disproportionate stress on lumbar discs, accelerating degeneration. Understanding these biomechanics informs both prevention strategies and surgical planning.
Degenerative CascadeFrom Healthy Disc to Painful Segment
The degenerative cascade in the lumbar spine often follows a predictable pattern. Understanding where a patient sits on this continuum informs treatment selection.

Early Biochemical Changes
Stage 1
Loss of proteoglycans and water. No major radiologic changes.
Treatment Consideration
Conservative management usually successful
Why Timing Matters for Disc Replacement
Earlier (Stage 2–3)
Disc pathology is dominant, facets relatively preserved.
Later (Stage 4–5)
Facets, ligaments, and alignment are badly affected.
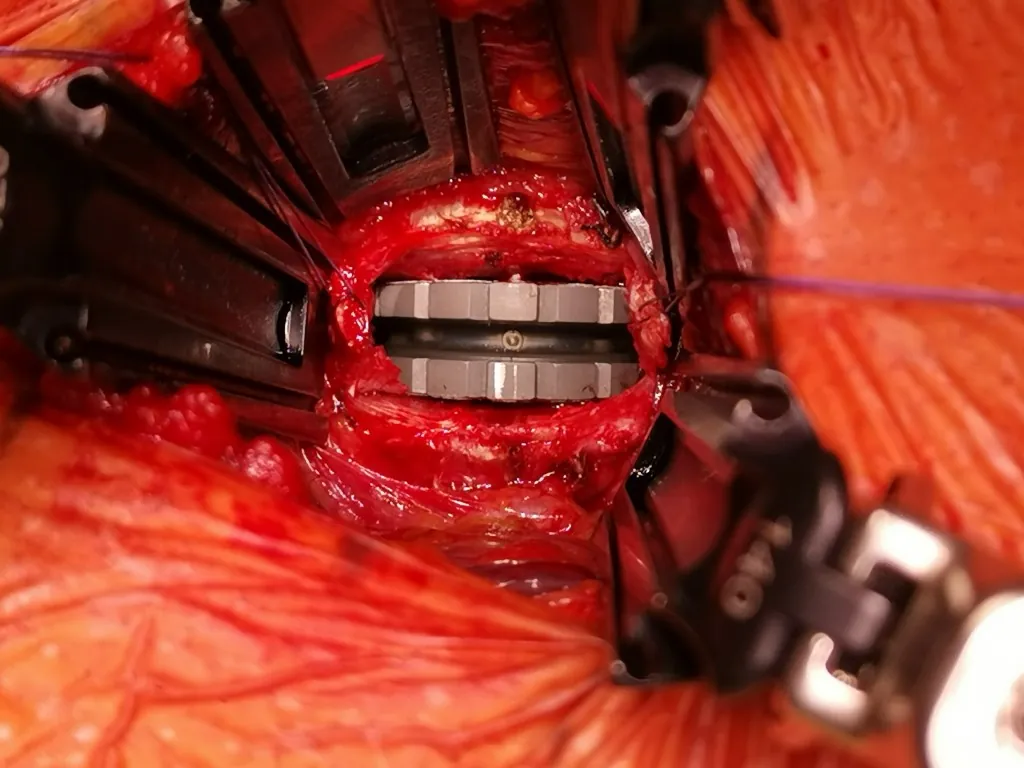
How Disc ReplacementRestores Function
Lumbar disc replacement (arthroplasty) addresses root causes of pain while preserving natural motion — offering a biomechanically superior alternative to fusion for appropriate candidates.
Remove Pain Generator
Excision of pathologic disc and herniated material that causes pain
Decompress Neural Structures
Relief of pressure on nerve roots and cauda equina
Restore Disc Height & Alignment
Re-establish proper spacing and spinal curvature
Preserve Segmental Motion
Maintain natural movement rather than eliminating it
Restoring Disc Height & Foraminal Space
Normal Disc
Degenerated Disc
After Disc Replacement
When an artificial disc restores height, intervertebral foramina enlarge (relieving nerve root compression), facet load normalises, and ligament tension is restored.
Disc Replacement vs Traditional Fusion
Long-Term Biomechanical Advantage
Evidence suggests that over 5–15 years, fusion segments may accelerate degeneration at levels above/below Disc replacement better preserves global lumbar mechanics and may reduce the need for future adjacent-level surgery in well-selected patients.
Clinical AnatomySymptoms & Levels
Matching dermatomal patterns, reflex changes, and weakness with imaging helps confirm the symptomatic level and guide surgical planning.
L5 Radiculopathy
L4–L5 disc involvement
Pain Distribution
Lateral thigh/leg, dorsum of foot
Weakness
Dorsiflexion, great toe extension
Reflex
Usually normal
Common Complaint
Foot drop or tripping over toes
Diagnostic Correlation
The symptom pattern plus imaging identifies which disc is responsible. Successful disc replacement requires decompression of the relevant nerve root and restoration of foraminal height.
Anatomical PrinciplesFor Successful Lumbar Arthroplasty
To optimise outcomes, surgeons must respect several key anatomical and biomechanical principles throughout the treatment planning and surgical process.

Better Outcomes When
- Symptoms map cleanly to one or two levels
- Imaging confirms focal disc pathology with preserved facets
- Overall alignment and bone quality are good
- Surgical planning respects detailed anatomy
More Complex Situations
- Multiple level degeneration
- Advanced facet arthrosis
- Significant spondylolisthesis or deformity
- Prior lumbar surgery (scar, altered anatomy)
- Severe osteoporosis or systemic disease
These scenarios may still be treatable — but often require fusion, hybrid constructs, or custom strategies rather than isolated arthroplasty.
Biomechanical VariationsWhy L4-L5 and L5-S1 Are Different
Understanding the anatomical and biomechanical differences between lumbar levels is essential for surgical planning and implant selection.
L4–L5 Segment
Sacro-Iliac Joint Considerations
The SI joints connect the sacrum to the pelvis and play a crucial role in load transfer
The Integrated Lumbar SpineEngineering of Load-Bearing
The lumbar spine is a load-transfer machine — a remarkable feat of biological engineering evolved to support your body's heaviest demands.
Five Vertebrae & Four Discs
Create a stacked column for axial load bearing
Posterior Facet Joints
Act as rails, guiding and limiting motion
Ligaments & Muscles
Provide active and passive restraint
Nerve Roots
Branch from cauda equina, organising sensation and motor control
When a Lumbar Disc Fails
Through degeneration, herniation, or collapse — the entire system is compromised:
Load redistribution → facet joints overloaded → arthritis
Height loss → foramina narrow → nerve root compression
Instability → excessive shear and abnormal motion → pain and stress on adjacent segments
How Disc Replacement Restores This System
Lumbar arthroplasty works because it addresses the root causes of disc failure. Select each benefit below to see the anatomical details:
By Understanding This Anatomy, You Now Appreciate
This Knowledge Empowers You To
Have informed discussions with your healthcare team
Understand your MRI findings and clinical examination
Appreciate the goals and benefits of motion-preserving surgery
Make evidence-based decisions about your spine care
“Your lumbar spine is an engineering marvel that has evolved to support your body's heaviest demands. Understanding its architecture, function, and pathology is the foundation for informed decision-making about your back health and future quality of life.”