
Lumbar Preoperative Assessment Patient Evaluation
The systematic clinical, diagnostic, and vascular evaluation process that determines whether you are a suitable candidate for lumbar disc replacement, what needs to be done surgically, and how to minimise risks and optimise outcomes.
Assessment Timeline
Comprehensive Evaluation
6–12 Weeks
Complete preoperative assessment from initial consultation through multidisciplinary review, vascular evaluation, and surgical optimisation.
Safety First
Critical Collaboration
Vascular
Mandatory vascular surgery collaboration for anterior approach ensuring optimal vessel safety and approach selection.
Patient Selection
Optimal Outcomes
Accuracy
Rigorous candidacy criteria ensuring only the most suitable patients proceed to surgery for superior long-term results.
Why Lumbar Preoperative AssessmentIs Different
The lumbar spine presents unique assessment challenges compared to cervical surgery. Understanding these differences helps you appreciate why your evaluation involves multiple specialists and typically requires 6–12 weeks from initial consultation to surgery.
Seven Key Differentiators
Vascular proximity
Lumbar approaches bring the surgeon near major vessels (aorta, iliac vessels, vena cava). Vascular complications are more common than in cervical surgery (1–3% vs. 0.5–1.5%).
Load-bearing role
The lumbar spine carries much greater axial loads. Biomechanical assessment and optimisation are more critical for long-term success.
Higher degeneration risk
Most humans experience some lumbar disc degeneration by age 60. Distinguishing pathological from incidental findings is crucial.
Adjacent-segment disease
Lumbar fusion has higher adjacent-segment degeneration rates (40–50% at 10 years) than cervical. Motion-preservation benefit is more significant long-term.
Functional limitations
Low back pain affects walking tolerance, sitting duration, and lifting capacity. Functional assessment is key to surgical planning.
Neurological patterns
Cauda equina involvement vs. single nerve root compression. Multilevel pathology is more common in the lumbar spine.
Psychological factors
Chronic low back pain often has a psychological component. Assessment is critical for outcome prediction and postoperative success.
The Assessment Timeline
Comprehensive assessment ensures optimal surgical outcomes
Initial Consultation
Comprehensive low back pain history and physical examination
Clinical Evaluation FrameworkFor Lumbar Pathology
Lumbar pain presentation is often complex. Detailed characterisation is essential to localise the problem, guide decisions, and predict surgical response.

Systematic Assessment
From symptom characterisation through comprehensive physical examination
Chief Complaint & Symptom Characterisation
Low Back Pain Characteristics
Why This Detail Matters
L5 vs L4 radiculopathy vs facet pain diagnosed by specific patterns
Severe disability may warrant earlier surgery; mild limitation may warrant continued conservative care
Good response to ESI suggests nerve root is pain generator; poor response raises diagnostic concerns
Physical Examination: The Lumbar Protocol
Inspection & Posture
Visual assessment of stance, gait, and overall presentation
| Muscle/Movement | Nerve Root | How to Test |
|---|---|---|
| Hip flexion | L2–L3 | Resist lifting leg straight up while sitting |
| Knee extension | L3–L4 | Resist straightening leg from bent position |
| Ankle dorsiflexion | L4–L5 | Resist pulling toes upward |
| Great toe extension | L5 | Resist pulling big toe upward (specific L5 test) |
| Ankle plantarflexion | S1 | Resist pushing foot downward (tiptoe walking test) |
| Hip abduction | L5 | Resist spreading legs apart |
| Intrinsic foot muscles | S1 | Assess toe spreading, foot intrinsic strength |
Sensory Testing (Light Touch, Pinprick)
Bilateral leg pain, saddle anaesthesia, loss of bladder/bowel control
History of cancer, unexplained weight loss, night pain, progressive neurological deficit
Fever, IV drug use, immunocompromised, recent spinal procedure
Recent trauma, significant osteoporosis, on long-term steroids
Claudication symptoms (exertional), absence of pain at rest initially
Red flags warrant urgent imaging and specialist consultation before elective surgery planning.
Diagnostic Imaging HierarchyStandard Imaging Modalities
A structured approach to imaging ensures we gather all necessary information for surgical planning while correlating findings with your clinical presentation.

Imaging Hierarchy
X-ray, MRI, CT, and CTA—each with specific diagnostic value
MRI Scan
Soft Tissue Gold Standard
Magnetic resonance imaging is the cornerstone of disc assessment, providing detailed visualisation of disc structure, hydration, and neural elements.
Key Imaging Principles
Clinical Correlation
Imaging findings must correlate with clinical symptoms. "Abnormal" MRI findings are common in pain-free individuals.
Weight-Bearing Assessment
Standing X-rays show true spinal alignment under load—different from supine imaging.
Multimodal Approach
X-ray, MRI, and CT each provide different information. The combination builds a complete picture.
Recent Imaging
Imaging should be within 6–12 months of surgery for accurate surgical planning.
Advanced Diagnostic ModalitiesBeyond Standard Imaging
When standard MRI and CT don't provide definitive answers, advanced diagnostic technologies can distinguish painful pathology from incidental findings and guide precise surgical planning.
Advanced Diagnostics
SPECT/CT, DEXA, Nociscan, and specialised testing for complex cases
SPECT/CT
Metabolic Activity Imaging
Single Photon Emission CT fused with CT reveals bone metabolic activity—which joints are actively inflamed versus inactive.
How It Works
When It's Indicated
Advantages
| T-Score | Classification | Arthroplasty Candidacy |
|---|---|---|
| > -1.0 | Normal bone | Excellent |
| -1.0 to -2.5 | Osteopenia | Good |
| -2.5 to -3.5 | Moderate osteoporosis | Questionable |
| -3.5 to -4.0 | Severe osteoporosis | Marginal |
| < -4.0 | Very severe osteoporosis | Contraindicated |
Management if osteoporosis found: Bone-strengthening medications (bisphosphonates, denosumab, teriparatide) can be started 3–6 months before surgery. Repeat DEXA shows if improvement sufficient for arthroplasty candidacy.
MRI shows herniations at L3-L4, L4-L5, L5-S1. Patient has generalised low back pain; unclear which level causes pain.
Nociscan Results:
Better outcomes than treating all herniations blindly
Nociscan MRI Spectroscopy
Traditional Discography
Current Status: Discography is becoming less common because of high false positive rates, invasive risks, and emerging non-invasive alternatives like Nociscan that provide similar or better information without complications.
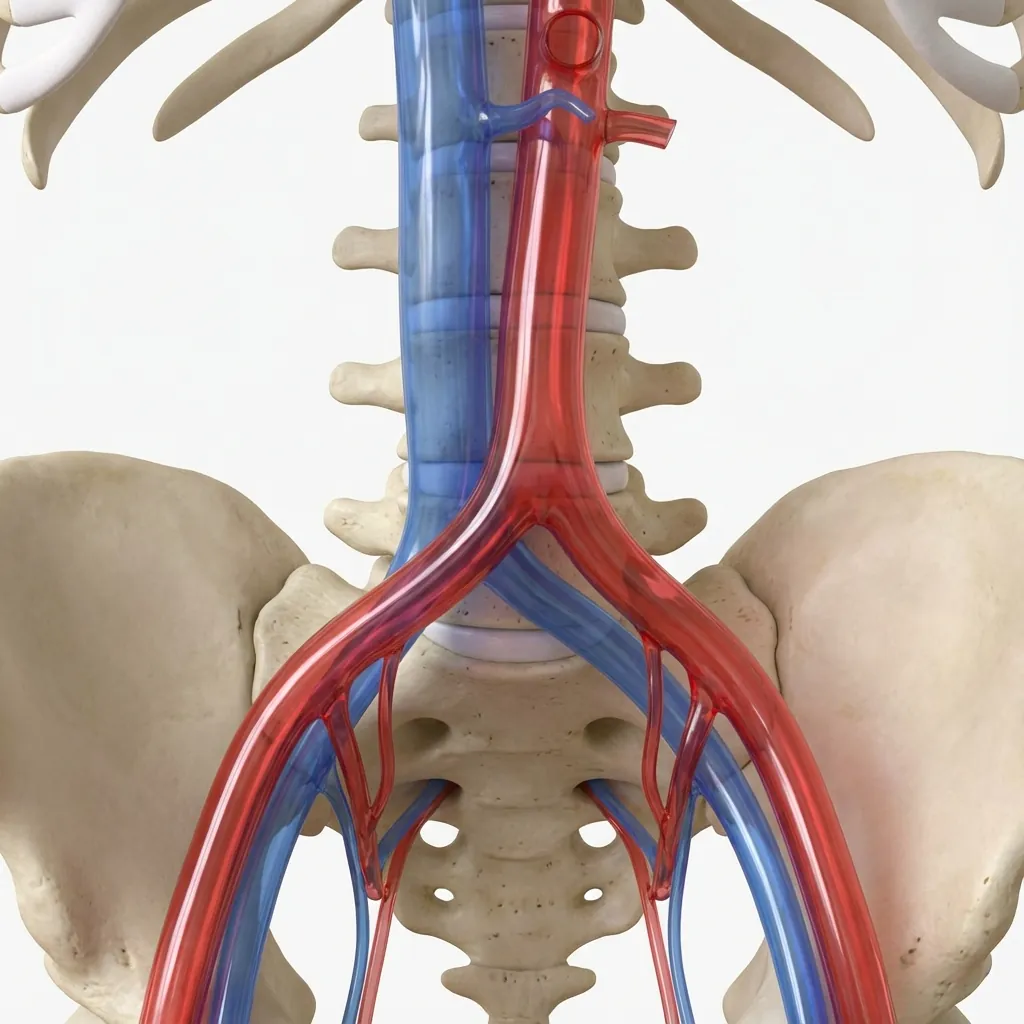
Vascular Surgery CollaborationIn Lumbar Disc Replacement
Lumbar disc replacement, particularly via the anterior approach, requires vascular surgeon expertise and collaboration. This partnership ensures optimal safety when operating near the body's major blood vessels.
Vascular Roadmap
CTA imaging maps vessel position relative to surgical targets
Why Vascular Surgeons Are Essential
Surgical Approach Proximity
Anterior approach brings the surgeon within millimetres of major vessels (aorta, vena cava, iliac vessels).
Real Complications
Though rare, vascular injury during lumbar spine surgery can be life-threatening and require immediate repair.
Underlying Vascular Disease
Aortic atherosclerosis, aneurysm, or prior vascular surgery changes the surgical risk profile significantly.
Vascular Surgery Assessment Process
Imaging Review
Risk Stratification
Approach Selection
Retraction Strategy
Need for Vascular Intervention
Anticoagulation Management
Collaboration on the Day of Surgery
When the vascular surgeon is involved in the surgical procedure
Communication between surgical teams: Position patient safely (avoid compression of vessels), communicate retraction needs and tolerances, establish plan if vascular injury occurs (direct repair vs. urgent vascular team notification).
Patient Selection CriteriaFor Lumbar Disc Arthroplasty
Not every patient with lumbar disc problems is a candidate for disc replacement. Careful selection ensures optimal outcomes and avoids complications in those better suited to fusion or conservative care.
Detailed Patient Selection
Rigorous criteria ensure the right procedure for each individual
Ideal Candidates for Lumbar Disc Arthroplasty
Patients meeting these criteria typically have excellent outcomes
Clinical Decision Guidance
Patient selection is individualised. Some patients with relative contraindications can become excellent candidates after appropriate optimisation (weight loss, smoking cessation, bone strengthening). Your surgeon will discuss your specific situation and determine if disc replacement, fusion, or continued conservative care is the most appropriate path.
Comorbidity ScreeningSystem-by-System Assessment
We screen for conditions that might affect surgical safety or outcome. This ensures optimal preparation and allows us to modify the surgical plan if needed.
Holistic Health Assessment
Eight major body systems evaluated for surgical readiness
Cardiovascular Assessment
The most critical preoperative assessment. Cardiac events are a major cause of perioperative morbidity.
Screening Questions
If significant cardiac disease, may need surgery at hospital with full cardiac backup, or optimisation (stent, medication adjustment) before elective surgery.
Multidisciplinary TeamCollaboration
Lumbar disc replacement is a team effort. Multiple specialists work together to ensure safe surgery and optimal outcomes.

Expert Collaboration
Five core surgical team members working together for your care
Core Surgical Team
Spine Surgeon (Orthopaedic or Neurosurgical)
Primary surgeon performing the disc replacement procedure
Key Responsibilities:
Cardiology
If significant cardiac history (prior MI, heart failure, arrhythmias)
Pulmonology
If moderate-severe COPD, poorly controlled asthma
Endocrinology
If poorly controlled diabetes (HbA1c >9%) or thyroid disease
Psychology / Pain Medicine
If chronic opioid use, depression, anxiety, or pain catastrophising
Haematology
If on complex anticoagulation or bleeding history
For complex cases—multilevel disease, significant comorbidities, prior spinal surgery, or borderline candidacy—a formal multidisciplinary team (MDT) meeting may be held where all relevant specialists review your case together.
Multiple experts contribute to the surgical plan, ensuring all angles are considered
Potential complications are identified early and mitigation strategies planned
All specialists aligned on timeline, goals, and postoperative expectations
Evidence shows multidisciplinary planning improves surgical outcomes
Case presentation includes: Complete history, imaging review, specialist recommendations, patient goals, and discussion of surgical options (arthroplasty vs. fusion vs. continued conservative care).
Functional & Activity AssessmentEstablishing Your Baseline
Understanding your current functional capacity helps us set realistic recovery goals and measure your improvement after surgery.

Baseline Metrics
Walking, sitting, standing tolerance and daily activity assessment
Key Functional Metrics
Walking Tolerance
Key Assessment Question
"How far can you walk before pain forces you to stop?"
Response Categories:
A structured walking program before surgery improves cardiovascular reserve, muscle strength, and mental readiness. This makes recovery faster and reduces complications.
Establish baseline
Gradual increase
Building endurance
Peak preparation
Core Stabilisation Exercises
Combined with walking, these exercises prepare your core for surgery and recovery:
Gentle contraction of deep abdominal muscles without breath-holding
Lying flat, gently flatten lower back against floor by tilting pelvis
On hands and knees, extend opposite arm and leg while maintaining stable spine
Lying on back with knees bent, lift pelvis keeping spine neutral
Why Baseline Matters
Your preoperative functional baseline becomes your comparison point for recovery. A 50% improvement in walking tolerance is more meaningful when we know you started at 200 metres and can now walk 300 metres. These objective measures help us track your success beyond subjective pain scores.
Shared Decision-MakingYour Treatment Options
Surgery is one option on a spectrum of treatments. Understanding all options—and the risks and benefits of each—helps you make an informed choice that aligns with your goals and values.

Treatment Pathway
From conservative care to surgical options
The Treatment Ladder
Most patients begin with conservative care, progressing to more invasive options only when simpler treatments have failed. Surgery is usually considered after 6 months of appropriate non-surgical treatment.
Conservative Care
First-Line Treatment
Interventional Procedures
Diagnostic & Therapeutic
Surgical Options
When Conservative Care Fails
Disc Arthroplasty
Replaces damaged disc with artificial disc that preserves motion
Spinal Fusion
Eliminates motion by fusing vertebrae together with bone graft
Reoperation Rates at 10 Years
Arthroplasty
Fusion
Overall Serious Complication Rate
Comparable to Hip/Knee replacement
The Shared Decision
Your surgeon will present the options, risks, and expected outcomes based on your specific situation. The final decision is made together—considering your goals (return to work, sports, daily activities), your values (willingness to accept risk, importance of motion preservation), and your life circumstances. There is no single "right" answer—only the right answer for you.
Preoperative OptimisationSetting You Up for Success
The weeks before surgery are an opportunity to actively improve your surgical outcome. Optimising your health reduces complications and speeds recovery.

Optimisation Program
Six key areas for preoperative preparation
Physical Therapy Program
Builds strength and endurance for surgery and recovery
Target Metrics
Increase by 50% from baseline
Hold plank for 30+ seconds
Walk 20 minutes without stopping
Optimisation Timeline Summary
- Stop smoking
- Begin PT program
- Start weight loss
- Optimise HbA1c/BP
- Nutrition supplements
- Psychological prep
- Final labs/imaging
- Medication review
- Pre-op visit
Final Assessment SynthesisBringing It All Together
All assessment components are synthesised to determine candidacy, approach, and surgical plan. This comprehensive review ensures optimal outcomes.

Comprehensive Review
Six assessment domains synthesised for surgical planning
Assessment Domain Review
Candidacy Determination
Excellent Candidate
All criteria met, optimal timing for surgery
Good Candidate (Optimisation Needed)
Candidate with modifiable factors requiring attention
Marginal Candidate
Significant concerns requiring careful consideration
Not a Candidate
Absolute contraindications or better alternatives exist
Once candidacy is confirmed, the surgical team meets to finalise the operative plan. This ensures all team members are aligned on approach, technique, and contingencies.
Surgical Approach
Levels to Address
Implant Selection
Intraoperative Monitoring
Anaesthesia Plan
Documentation
Administrative
Laboratory
Laboratory
Imaging
Equipment
Medications
Medications
Preparation
Preparation
Logistics
Discharge
Ready for Surgery
Once all assessment components are complete and optimisation targets are met, you're ready for surgery. Your surgeon will confirm the date, provide final instructions, and answer any remaining questions. The journey from preoperative assessment to surgical readiness is complete—now it's time to focus on recovery and achieving your goals.