Professional Collaboration Expert Partnership
Professional medical collaboration and referral network for neurosurgical consultations. Comprehensive care coordination with referring physicians ensuring seamless patient care and optimal treatment outcomes through multidisciplinary expertise.
Care Coordination
Integrated Care
Seamless
Comprehensive care coordination with referring physicians ensuring continuity of care and optimal patient outcomes throughout treatment journey.
Neurosurgical Care
Specialized Treatment
Expert
Internationally trained neurosurgical expertise ensuring patients receive the highest standard of specialized spine care and treatment.
Communication
Professional Access
Direct
Direct communication channels with referring doctors ensuring timely updates and coordinated care planning throughout patient treatment.
Comprehensive Clinical InformationFor Evidence-Based Motion-Preserving Surgery
This professional resource provides healthcare providers with detailed, evidence-based information regarding patient selection criteria, diagnostic requirements, clinical outcomes, and procedural details for cervical and lumbar disc replacement procedures.
Disc replacement surgery represents a paradigm shift in the treatment of symptomatic degenerative disc disease, offering superior long-term outcomes compared to spinal fusion in appropriately selected patients.
Dr Aliashkevich welcomes referrals from healthcare professionals and is committed to collaborative care ensuring optimal patient outcomes.
Clinical Philosophy
“As a strong advocate for motion-preserving spinal surgery, I recommend considering disc replacement as the preferred choice over fusion. Only when disc replacement is not feasible—due to anatomic constraints, severe pathology, or other factors—should consideration be given to fusion or hybrid procedures combining disc replacement at one level with fusion at another.
Cervical Disc ReplacementPatient Selection Criteria
Rigorous patient selection is fundamental to excellent outcomes. Use the tabs below to explore clinical indications, diagnostic requirements, and eligibility criteria.
Symptomatic Degenerative Disc Disease
Chronic neck pain, cervical radiculopathy, or myelopathy directly attributable to an intervertebral disc with corresponding imaging findings.
Radicular Pain Patterns
Intractable shoulder, arm, hand, or finger pain with clear dermatome distribution and nerve root compression on imaging, indicating cervical nerve root involvement.
Neurological Deficits
Tingling, numbness, weakness in arms or hands, loss of fine dexterity, balance disturbances, or gait abnormalities causally related to the spinal pathology.
Failed Conservative Therapy
Comprehensive non-surgical treatment trial of at least 6 weeks to 3 months, ideally 6+ months, including rest, medications, physiotherapy, and potentially spinal injections.
Functional Impairment
Pain and neurological symptoms sufficiently severe to impair work capacity, recreational activities, or quality of life despite conservative management.
Lumbar Disc ReplacementPatient Selection Criteria
Lumbar disc replacement requires additional considerations including vascular assessment and multidisciplinary surgical team collaboration for optimal outcomes.
Chronic Back Pain with Radiculopathy
Back pain combined with leg pain suggesting nerve root involvement from intervertebral disc pathology.
Failed Conservative Treatment
Documented trial of comprehensive non-surgical management for minimum 6 months, including medical therapy, physiotherapy, and potentially spinal injections.
Intractable Radicular Leg Pain
Leg pain severe enough to significantly impair function and quality of life, with neurological deficits or imaging evidence of compression.
Functional Impairment
Pain-related limitations affecting work, recreational activities, or activities of daily living despite conservative management.
Young Patient Age
Disc replacement particularly advantageous in younger patients who would benefit from motion preservation over decades.
Comprehensive Diagnostic RequirementsEvidence-Based Imaging Protocols
Accurate diagnosis requires a systematic approach to imaging and testing. Each modality provides specific information essential for surgical planning.

Essential Imaging Studies
Additional Studies (When Indicated)
Electromyography (EMG) & Nerve Conduction Studies (NCS)
Diagnostic uncertainty or multilevel disease
Confirms nerve root involvement and localises compression level
Somatosensory Evoked Potentials (SSEP)
Myelopathy suspected
Evaluates spinal cord function and conduction
Diagnostic Nerve Root Blocks
Multiple levels of compression or ambiguous presentation
Confirm symptomatic nerve root via >50% pain relief
Provocative Discography
Suspected discogenic pain without clear nerve compression
Identify primary pain generator
SPECT-CT Imaging
Multiple levels involved or suspected facet/SI joint pathology
Identifies areas of active inflammation
Imaging Documentation for Referral
When referring, please provide imaging on CD or electronic format for detailed review. Include radiology reports and highlight specific images most relevant to the clinical question (oblique cervical foraminal views, flexion-extension radiographs, vascular imaging for lumbar cases).
Comprehensive Non-SurgicalTreatment Prerequisites
Disc replacement should be reserved for patients who have genuinely failed comprehensive conservative management. The following represents the expected minimum conservative treatment trial.

Why Conservative Treatment Matters
Many patients improve significantly with appropriate conservative management. Surgery is reserved for those who have genuinely exhausted non-operative options and continue to experience significant symptoms affecting their quality of life.
Referral Documentation
When referring, please include comprehensive documentation of conservative treatment attempts:
Treatment Timeline
Dates, frequency, and duration of all therapies
Response Assessment
Objective measures of treatment response
Failure Documentation
Clear rationale for conservative treatment failure
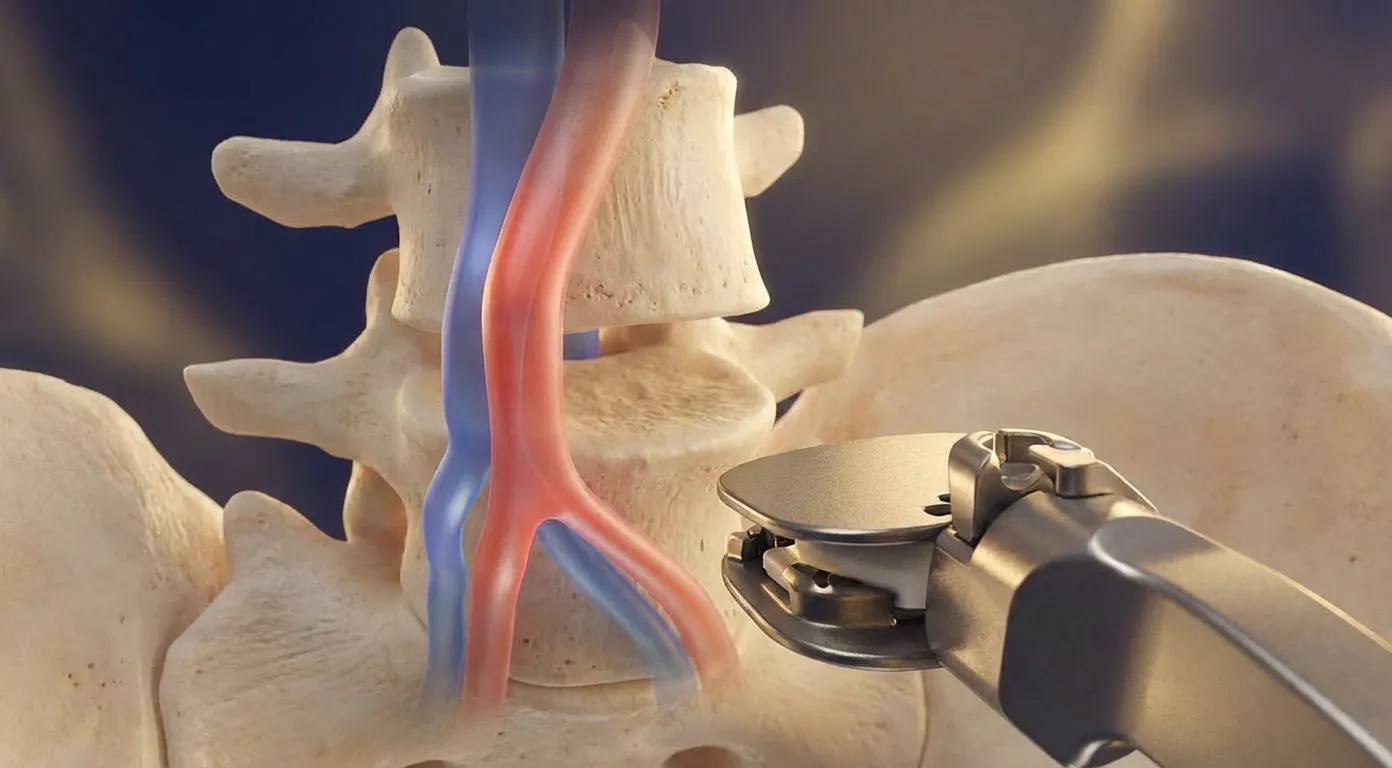
Surgical Technique& Procedural Details
Both cervical and lumbar disc replacement utilise anterior approaches, providing direct access to the pathology with minimal muscle disruption.
Cervical Disc Replacement
Anterior Cervical Approach
The anterior cervical approach is the standard method for accessing cervical intervertebral discs, allowing direct visualization and minimal soft tissue trauma.
Key Procedural Elements
Surgical Advantages
Lumbar Disc Replacement
Anterior Retroperitoneal Approach
The anterior retroperitoneal approach avoids abdominal organs and peritoneal cavity, incorporating vascular surgeon collaboration for safe anterior access.
Key Procedural Elements
Surgical Advantages
Both procedures represent the culmination of decades of surgical refinement, combining motion preservation with neural decompression for optimal patient outcomes.
Clinical Outcomes& Evidence-Based Results
Multiple investigations spanning 15+ years consistently demonstrate superior patient outcomes with disc replacement compared to fusion in appropriately selected candidates.
Comparative Outcomes: Disc Replacement vs Fusion
Patient Satisfaction
vs 70–80% with fusion
ASD Risk Reduction
Lower reoperation for adjacent segment disease
Motion Preserved
Sustained over 10+ years follow-up
Pain Relief
Return to Activities
Extremely Low Complication Rates
Clinical data from University of Toronto and other major academic centres' long-term studies with follow-up extending beyond 14 years confirms sustained superiority of motion preservation.
Implant Technology& Selection Criteria
Modern disc replacement implants represent decades of biomechanical research, offering reliable motion preservation designed to last throughout the patient's lifetime.

Implant Materials
Implant Selection Criteria
Patient Factors
Surgeon Factors
Level-Specific
Modern implants are designed for 40–70 years of reliable function, with clinical data from 13–14 year follow-up showing zero mechanical failures requiring device removal.
Proven Track RecordIn Motion-Preserving Surgery
Nearly three decades dedicated to specialising in motion-preserving spinal surgery, with extensive experience across diverse patient populations and complex surgical scenarios.

Clinical Experience Timeline
Neurosurgery Career Begins
Joined The Belarusian Scientific and Research Institute of Neurology, Neurosurgery and Physiotherapy
Cervical Disc Replacement
19+ years of cervical arthroplasty experience with hundreds of procedures completed
Lumbar Disc Replacement
13+ years of lumbar arthroplasty with excellent surgical outcomes
Comprehensive Expertise
Multilevel disease, hybrid procedures, revision cases, and complex presentations
Clinical Philosophy
Motion Preservation as Best Practice
“As a strong advocate for motion-preserving spinal surgery, I recommend considering disc replacement as the preferred choice over fusion. Only when disc replacement is not feasible—due to anatomic constraints, severe pathology, or other factors—should consideration be given to fusion or hybrid procedures combining disc replacement at one level with fusion at another.”
This philosophy is not dogmatic, but rather reflects the cumulative evidence from multiple prospective comparative studies, meta-analyses, and long-term follow-up investigations demonstrating the superior long-term outcomes of motion preservation.
Evidence-Based Outcomes
Outcome Parameters Favouring Disc Replacement
Comprehensive Surgical Expertise
Single-Level Procedures
Standard cervical and lumbar disc replacement with excellent outcomes and low complication rates.
Multilevel Disease
Complex presentations requiring multiple levels of treatment with tailored surgical planning.
Hybrid Procedures
Combination of disc replacement and fusion when indicated by pathology at different levels.
Revision Cases
Complex revisions and patients with significant preoperative neurological compromise.
Clinical studies with 13–14 year follow-up demonstrate that modern disc replacement implants maintain excellent function throughout the patient's lifetime, with zero mechanical failures requiring device removal reported in the longest series.
Referral Process& Communication
A streamlined referral process ensures efficient patient care and clear communication between referring physicians and our practice.
Referral Workflow
Essential Referral Documentation
Medical History
Imaging Studies
Clinical Findings
Consultation Report
Detailed consultation report provided within 48 hours including:
Ongoing Communication
Maintained throughout the patient journey:
Patient Expectations& Recovery Timelines
Setting realistic expectations is crucial for patient satisfaction. Understanding typical recovery timelines helps patients plan their return to normal activities.

Success Rates
Recovery Timeline Comparison
Long-Term Activity Capacity
Temporary Restrictions
Medication Expectations
Motion Preservation Benefits
For younger patients with decades of life remaining, these differences translate into meaningful reductions in cumulative reoperation risk and sustained functional capacity.
Referral Contact& Professional Inquiries
Dr Aliashkevich welcomes referrals from healthcare professionals and is committed to collaborative care ensuring optimal patient outcomes.

Making a Referral
Professional Development
Frequently Asked Questions for Professional Referrers
Motion preservation provides multiple advantages: 50–67% reduction in adjacent segment disease requiring reoperation, higher patient satisfaction rates (85–95% vs 70–80%), faster return to work, lower overall reoperation rates (5–6% vs 7–26%), and elimination of fusion-related complications such as pseudarthrosis and adjacent segment disease acceleration. For younger patients with decades of life remaining, these long-term benefits are clinically significant.
Individual assessment considers multiple factors: number of levels with pathology, severity of pathology at each level, bone quality, facet joint status, patient age, and patient goals. Single-level disc replacement is performed when a single level is symptomatic and meets selection criteria. Hybrid procedures (disc replacement at one level, fusion at another) are utilised when two-level disease is present with different characteristics at each level, or when one level has contraindications to disc replacement but the other is ideal for replacement.
Hospital stay is typically 1–2 nights for cervical procedures and 2–4 nights for lumbar procedures. Return to light work (sedentary) occurs within 2–4 weeks for cervical and 4–6 weeks for lumbar procedures. Return to full work duties is typically 4–8 weeks for cervical and 6–12 weeks for lumbar procedures, depending on occupational demands. Complete functional recovery typically requires 3–6 months, with continued improvement possible beyond this timeframe.
Experienced vascular surgeon collaboration provides expertise in managing the anterior lumbar approach where major vessels (aorta, vena cava, iliac vessels) are closely related. The vascular surgeon assists with preoperative vascular imaging analysis, intraoperative vascular isolation and retraction, and management of any vascular complications. This multidisciplinary approach significantly reduces the risk of major vessel injury, which is the most serious potential complication of lumbar disc replacement.
Modern implants are designed for 40–70 years of reliable function, with the expectation that they will function throughout the patient's lifetime for most patients. Clinical data supporting this comes from 13–14 year follow-up studies showing zero mechanical failures requiring device removal, and biomechanical studies suggesting implants could function 40+ years. The stress profile experienced by spine implants is actually lower than experienced by hip and knee replacements, which have proven 20+ year durability in routine clinical practice.
Rigorous patient selection is fundamental to excellent outcomes. Ideal candidates have single-level symptomatic pathology with clear imaging-clinical correlation, preserved disc height and mobility, adequate bone quality, no significant facet joint arthropathy, failed conservative therapy, and realistic expectations. Contraindications (osteoporosis, instability, severe facet disease, etc.) are carefully assessed. Additionally, individual factors such as age, medical comorbidities, occupational demands, and patient goals influence suitability for disc replacement versus alternative approaches.
Realistic discussion centres on 85–95% satisfaction rates in appropriately selected patients, with 85–90% achieving substantial pain relief (>50% improvement), and 50–60% achieving near-complete pain resolution. Return to work is expected in 80–90% by 3 months. Patients should understand that outcomes vary individually, and that partial pain relief with functional restoration and return to valued activities represents successful surgery. Discussion should include realistic timelines (3–6 months for full recovery) and temporary activity restrictions. Comparative data demonstrating superiority to fusion should be presented.
Commitment to Collaborative Care
Evidence-Based Practice
Latest research integration into clinical practice
Continuous outcome monitoring to refine practice
Shared decision-making respecting patient preferences
Transparency regarding risks, benefits, alternatives
Transparent Communication
Detailed reports to referring physicians
Prompt communication regarding patient progress
Immediate notification if complications develop
Collaboration on postoperative management
Collaborative Care Model
Respect for existing physician-patient relationships
Shared responsibility appropriate to expertise
Return of patient to referring physician for ongoing care
Consultation availability for questions and complications
Continuous Improvement
Systematic follow-up assessing outcomes
Identification and analysis of complications
Ongoing refinement of surgical technique
Integration of patient feedback
Thank you for considering Dr Aliashkevich for your patients requiring motion-preserving spine surgery. We look forward to working collaboratively with you to achieve the best possible outcomes for your patients.
This professional resource provides evidence-based clinical information for healthcare providers. Individual patient assessment and clinical judgment remain essential for appropriate treatment recommendations.