Lumbar Disc Replacement History Decades Of Innovation
Comprehensive history of lumbar disc replacement technology from early steel sphere implants through modern viscoelastic disc systems. Understanding this evolution demonstrates the scientific foundation and proven track record of lumbar arthroplasty procedures.
First Implants
Pioneering Work
1960s
First attempts at lumbar disc replacement using steel sphere implants by Fernstrom, establishing the foundation for modern motion-preserving technology.
Modern Era
Refined Technology
1980s-90s
Development of modern lumbar disc replacement systems with improved materials, design features, and surgical techniques for better patient outcomes.
Advanced Systems
Current Standards
2024
State-of-the-art lumbar disc replacement systems with advanced biomechanical properties, improved longevity, and proven clinical outcomes for optimal patient care.
The Foundation EraEarly Spinal Surgery Pioneers
The recognition of disc herniation as a distinct clinical entity emerged in the 1930s, establishing the foundation for surgical interventions that would eventually evolve into motion-preserving technologies.

The Dawn of Modern Disc Surgery
Harvard Medical School, 1934 — Groundbreaking surgical treatment of lumbar disc herniation
Harvard Medical School, 1934
Mixter & Barr Publication
William Jason Mixter and Joseph Seaton Barr at Harvard Medical School published their groundbreaking work in 1934, describing the surgical treatment of lumbar disc herniation and establishing the foundational principles upon which all subsequent lumbar spine surgery would be built.
These early procedures focused exclusively on removing herniated disc material through posterior approaches, establishing the critical relationship between disc pathology and neurological symptoms. The posterior approach provided excellent access to neural structures at risk, allowing effective decompression but with limited ability to address the underlying discogenic pain generator.
However, the revolutionary concept of replacing rather than simply removing damaged disc tissue would not emerge for another three decades, awaiting advances in materials science, biomechanical understanding, and surgical technique development.
Pioneering Contributors
The Posterior Approach Legacy
These early techniques established the posterior approach to the lumbar spine that remains the foundation for many spinal procedures today, fundamentally demonstrating that surgical intervention could provide lasting relief from debilitating symptoms.
Foundational Principles Established
The early pioneers established several crucial principles that would later inform disc replacement development. These foundational principles guided all subsequent innovations in lumbar spine surgery:
The Fernström RevolutionFirst Attempts at Motion Preservation
Dr Ulf Fernström, a surgeon from Uddevalla, Sweden, deserves recognition as the true pioneer of artificial disc replacement. In 1959, inspired by successful hip and knee joint replacements, he conceived the revolutionary idea of maintaining spinal motion through disc replacement.

Stainless Steel Spheres
Adapted from industrial ball bearings for spinal use — a revolutionary concept
The Swedish Ball Bearing Factory Collaboration
Working in close collaboration with the Swedish Ball Bearing Factory, Fernström adapted standard industrial ball bearings for spinal use. His approach was elegantly simple yet profoundly groundbreaking: replace the degenerated disc with a solid stainless-steel sphere that would maintain disc height whilst permitting controlled spinal motion.
This visionary concept challenged the established fusion-based paradigm and anticipated modern motion-preserving principles by more than four decades.
Clinical Experience and Encouraging Early Results
Fernström's initial results appeared remarkably promising, with reported outcomes matching those of fusion procedures whilst preserving precious spinal mobility—the fundamental advantage envisioned by modern motion-preserving philosophy.
For herniation patients, persistent low back pain occurred in only 12% of cases compared to 60% in control patients treated with discectomy alone.
McKenzie, another early adopter inspired by Fernström's vision, implanted 155 Fernström Balls in 103 patients and reported excellent and good results in 85% of patients during short-term follow-up. Remarkably, long-term data extending to 17 years continued to demonstrate favourable outcomes.
Clinical Statistics
Lumbar Spheres Implanted
Patients Treated
Persistent Pain (Sphere)
Persistent Pain (Control)
Roentgenographic studies confirmed preservation of segmental motion at implanted levels, validating the fundamental motion-preserving principle that would later guide modern device development.
Despite initial enthusiasm and promising early results, the Fernström Ball era revealed fundamental limitations that reflected the incomplete understanding of spinal biomechanics available in the 1960s:
Subsidence and Material Incompatibility
The metal spheres progressively eroded into the softer vertebral endplates due to excessive contact pressures and the significant modulus mismatch between rigid steel (200 GPa) and living bone tissue (7-20 GPa).
Migration and Instability
Inadequate fixation mechanisms and the unconstrained spherical design led to device displacement and occasional complete extrusion from the disc space.
Hypermobility and Adjacent Segment Effects
The spherical design allowed excessive motion in all planes, creating instability rather than controlled mobility and abnormal stress patterns at neighbouring segments.
Biomechanical Incompatibility
The rigid steel construction could not replicate the crucial viscoelastic properties that define natural disc tissue as a remarkable shock absorber.
By the late 1960s, mounting complications and the acknowledged lack of sophisticated biomechanical understanding led to abandonment of the Fernström Ball concept. However, the fundamental principle of motion preservation had been permanently established in medical consciousness.
The Remarkable Fernström Legacy
In a fascinating historical twist, the Fernström concept experienced a brief resurgence in the early 2000s with the introduction of the cobalt-chromium-molybdenum sphere (Satellite Spinal System, Medtronic Sofamor Danek). This device received FDA approval in 2005 but was withdrawn in 2007 due to disappointing clinical performance.
Contemporary reports of revision surgeries powerfully reinforced the lessons learned from the original Fernström era: successful disc replacement demanded sophisticated understanding of spinal biomechanics and revolutionary advances in materials science beyond simple metallic spheres.
The German InnovationBirth of Modern Disc Replacement
The modern era of lumbar disc replacement began in East Berlin during the early 1980s with the development of the Charité Artificial Disc. This revolutionary device was conceived through the remarkable collaboration of Professor Dr Karin Büttner-Janz and Professor Dr Kurt Schellnack.

Charité Device Evolution
Three generations of systematic innovation through rigorous clinical experience
Professor Dr Karin Büttner-Janz
Olympic Champion & Medical Pioneer
Dr Karin Büttner-Janz represents one of medicine's most fascinating figures—an Olympic champion who achieved gold medals in gymnastics at the 1972 Munich Olympics before pursuing medical advancement.
Her extraordinary athletic background provided intuitive understanding of spinal motion and loading patterns that profoundly informed the design philosophy of the world's first successful artificial disc. Büttner-Janz's unique perspective as an elite athlete proved invaluable in conceptualising a device that could withstand complex physiological forces whilst maintaining natural motion characteristics.
SB Charité Evolution
SB Charité III
The definitive design featured precisely engineered cast cobalt-chromium-molybdenum (CoCrMo) alloy endplates with three anterior and three posterior anchoring teeth, providing optimal equilibrium between fixation strength and structural integrity.
Most significantly, despite substantial design differences between the three device generations, clinical outcomes remained consistently favourable, suggesting the fundamental motion-preserving concept was more important than specific engineering details.
Revolutionary Design Principles
Three-Component Architecture
Two metal endplates with a mobile polyethylene core elegantly replicated the basic structure of natural disc anatomy.
Unconstrained Motion Philosophy
The innovative free-floating sliding core allowed dynamic translation during spinal movement to mimic natural disc kinematics.
Advanced Load Distribution
The large endplate footprint effectively distributed mechanical loads, dramatically reducing contact pressures and subsidence risk.
Proven Biocompatible Materials
The sophisticated CoCrMo/UHMWPE combination drew from decades of successful joint replacement experience.
Clinical Development
The first SB Charité I was successfully implanted in 1984, initiating clinical experience that would span decades. Between 1984 and 1989, 71 consecutive patients received 84 Charité prostheses, providing the world's first systematic experience with modern disc replacement technology.
Remarkably, long-term follow-up studies extending to 17 years demonstrated maintained clinical benefit and preserved motion at implanted levels.
Global Impact
The Charité III was first marketed by Waldemar Link outside the United States in 1987. More than 15,000 prostheses were implanted worldwide prior to FDA approval, establishing an unprecedented database of international clinical experience.
DePuy Spine acquired product rights in 2004, coinciding with historic FDA approval and marking the beginning of widespread US adoption.
The American ExperienceFDA Regulation and Clinical Validation
Whilst lumbar disc replacement technology had accumulated substantial international experience, FDA approval in the United States required unprecedented levels of clinical validation through the rigorous Investigational Device Exemption (IDE) process.

Historic FDA Validation
Rigorous clinical evidence established the foundation for motion-preserving surgery in the US
The IDE Process
Investigational Device Exemption
The Investigational Device Exemption (IDE) process requires prospective, randomised, controlled clinical trials comparing new devices against established treatments. For lumbar disc replacement, this meant direct comparison with lumbar fusion—the existing gold standard.
This rigorous framework created the world's most comprehensive dataset for motion-preserving spinal technology, with outcomes extending to 5, 7, and eventually 10+ year follow-up periods.
Landmark Charité IDE Study
Prospective Randomised Trial
The historic Charité IDE study enrolled 304 patients across 14 specialised centres, randomising participants in a 2:1 ratio between disc replacement and anterior lumbar interbody fusion.
Primary endpoints included Oswestry Disability Index (ODI) improvement, visual analogue scale (VAS) pain scores, neurological status, and device-related complications—establishing the template for all subsequent device approvals.
Study Design Features
Historic FDA Milestones
Charité FDA Approval
First lumbar disc replacement approved in US for single-level use from L4-S1, based on extensive worldwide clinical experience
ProDisc-L FDA Approval
Alternative ball-and-socket design approved, representing different biomechanical philosophy from Charité's unconstrained sliding core
Multi-Level Approval
ProDisc-L received expanded approval for one or two contiguous levels from L3-S1
International DevelopmentGlobal Innovation and Alternative Approaches
Whilst the Charité pioneered the mobile-bearing concept, parallel development in France led to the ProDisc-L—representing a fundamentally different engineering philosophy that would prove equally influential in shaping modern disc replacement technology.

Worldwide Collaboration
Contributions from four continents shaped modern disc replacement technology
The ProDisc-L Development
Marnay & Bertagnoli Collaboration
Dr Thierry Marnay and Dr Rudolf Bertagnoli led the development of this ball-and-socket design, representing a fundamentally different approach from the Charité's unconstrained sliding core philosophy.
European clinical trials demonstrated favourable outcomes extending to 7-11 years post-operatively.
LP-ESP: Biomimetic Technology
The LP-ESP (Elastic Spine Pad) represents a revolutionary approach, developed through an intensive 20-year research programme. This innovative device incorporates aone-piece deformable implant with a silicone gel core surrounded by polycarbonate urethane.
Providing six degrees of freedom including crucial shock absorption, whilst advanced viscoelastic polymers more closely replicate natural disc properties including load distribution and energy return.
Variable Centre of Rotation
This innovative technology allows the rotation centre to vary freely during movement, more accurately replicating the complex motion patterns of healthy discs. Unlike fixed-pivot designs, the variable centre of rotation adapts dynamically to each patient's unique biomechanical demands.
Legacy of Global Collaboration
The evolution of lumbar disc replacement technology represents a remarkable story of international collaboration, with each nation contributing unique expertise and perspectives:
Sweden
Fernström visionary concept
Germany
Büttner-Janz engineering brilliance
France
Marnay-Bertagnoli ball-and-socket design
United States
FDA regulatory framework and commercial development
The Australian Regulatory JourneyTGA Framework and Clinical Standards
Australia's experience with lumbar disc replacement reflects the complex interplay between advancing clinical evidence, regulatory approval processes, and healthcare funding decisions—maintaining a sophisticated balance between innovation and patient safety.

Australian Medical Standards
Rigorous regulatory oversight ensuring patient safety and device quality
Medicare Coverage Evolution
Policy Framework
Unlike cervical disc replacement, which experienced a temporary Medicare withdrawal, lumbar disc replacement has maintained more consistent coverage through the comprehensive Medicare Benefits Schedule. This reflects genuine acceptance of motion-preserving technology in Australian healthcare.
Lumbar disc replacement procedures may be utilised for patients who meet specific clinical criteria:
TGA Regulatory Framework
Class III Reclassification
The Therapeutic Goods Administration (TGA) has implemented comprehensive regulatory reforms specifically addressing spinal implantable devices. From November 25, 2021, motion-preserving spinal devices were systematically reclassified from Class IIb to Class III medical devices.
This important reclassification reflects the inherently higher risk profile and increased complexity of motion-preserving devices compared to traditional fusion implants.
Enhanced Class III Requirements
Rigorous Clinical Evidence
Comprehensive safety and efficacy data required
Conformity Assessment
Mandatory documentation ensuring device quality and consistency
Post-Market Surveillance
Comprehensive monitoring of long-term performance and safety
Patient Information
Detailed requirements including mandatory implant identification cards
Single-Level Coverage and Hybrid Procedures
Australian Medicare currently restricts coverage to single-level procedures only, presenting a notable contrast with recent FDA approvals for multi-level procedures in the United States. This conservative approach reflects ongoing careful evaluation of clinical evidence for multi-level procedures.
Australia 🇦🇺
Single-level procedures only under Medicare
United States 🇺🇸
Multi-level approval since April 2020
Patients requiring multi-level treatment may be appropriate candidates for innovative hybrid procedures, which combine disc replacement at one level with fusion at adjacent affected levels—acknowledging the clinical reality of multi-level degenerative disease whilst maintaining strict adherence to evidence-based treatment protocols.
Contemporary Clinical EvidenceLong-Term Outcomes and RCT Data
The accumulated evidence from randomised controlled trials and long-term registry data now provides compelling support for motion-preserving surgery in appropriately selected patients, with outcomes extending to 10+ years of follow-up.
Evidence-Based Outcomes
Comprehensive RCT data supporting motion-preserving outcomes
Patient Satisfaction
≥10-year satisfaction rate (±6.97%)
Motion Preserved
Segmental motion range across devices
Adjacent Segment Protection
vs 28.6% for fusion at 10 years
Reoperation Rate
vs 18% for fusion at 5 years
Primary Outcome Measures
Functional Outcomes
Oswestry Disability Index (ODI) improvement matching or exceeding fusion outcomes at all follow-up points.
Motion Preservation
Maintained segmental motion averaging 4-6° at index level throughout long-term follow-up periods.
Adjacent Segment Protection
Reduced rates of adjacent segment degeneration compared to fusion patients in matched cohorts.
Reduced Reoperation
Lower index-level reoperation rates compared to fusion at 5, 7, and 10-year follow-up.
Pain Control Outcomes
Visual analogue scale (VAS) assessments demonstrate statistically significant and clinically meaningful improvements in both back pain and leg pain scores maintained throughout extended follow-up periods.
These improvements parallel functional gains measured by validated disability instruments, confirming that motion preservation provides durable pain relief without compromising clinical outcomes.
Biomechanical Validation
Finite element analysis demonstrates that lumbar fusion significantly increases intradiscal pressure at adjacent levels: flexion loads increase pressures by 45-73%, whilst extension increases segmental motion at adjacent levels by 35-45%.
In contrast, lumbar disc arthroplasty maintains normal stress distribution patterns at adjacent levels, with segmental motion remaining similar to intact specimens—providing scientific support for the clinical findings of reduced adjacent segment disease.
| Outcome | Disc Replacement | Fusion | Significance |
|---|---|---|---|
| Clinical Success (5yr) | 72.8% ± 15.15% | Baseline | RR 1.09-1.13 |
| Clinical Success (≥10yr) | 84.07% ± 9.99% | Baseline | Superior |
| VAS Back Pain | 8.6 → 1.6 | Similar reduction | MCID exceeded |
| VAS Leg Pain | 7.3 → 1.1 | Similar reduction | MCID exceeded |
| ODI Score | 46 → 27 | Similar | Clinically meaningful |
| Adjacent Segment (5yr) | 9-14% | 28-34% | p < 0.01 |
| Adjacent Segment (10yr) | 9.2% | 28.6% | p < 0.01 |
| Reoperation (5yr) | 7.83% ± 2.80% | ~18% | p < 0.05 |
| Return-to-Work | 9-14 days earlier | Baseline | Significant |
| Complete Pain Resolution | 52.3% | Not reported | 33% minimal only |
| Complication Rate (5yr) | 18.84% ± 6.82% | Similar | Expected |
| Complication Rate (≥10yr) | 27.2% ± 5.29% | Similar | Long-term |
Data compiled from pooled analysis of FDA IDE trials and international registry studies with minimum 5-year follow-up.
Lessons From HistoryPrinciples for Continued Success
The remarkable journey of lumbar disc replacement technology teaches us enduring lessons about medical device innovation, the importance of systematic development, and the value of international collaboration in advancing patient care.
The Path to Modern Success
Each generation of pioneers has contributed invaluable knowledge to our understanding of spinal biomechanics and the exacting requirements for successful motion preservation. From Fernström's visionary concept through Büttner-Janz's engineering brilliance to contemporary biomimetic designs, these lessons continue to guide the field toward ever-improving patient outcomes.
Iterative Development
The remarkable progression from Fernström's pioneering spheres through Charité evolution to contemporary sophisticated devices illustrates the inherently iterative nature of complex medical device development.
This evolutionary process requires unwavering commitment to scientific methodology, honest assessment of both successes and failures, and persistent refinement based on accumulating clinical evidence.
Biomechanical Understanding
Success in lumbar disc replacement correlates directly with advancing understanding of the incredibly complex biomechanics governing spinal function. Early failures reflected limited knowledge regarding load distribution patterns and material property requirements.
This evolution continues to accelerate, driven by advances in imaging technology, computational analysis, and materials science that enable ever-more-sophisticated device designs.
Regulatory Validation
The demanding FDA IDE process, whilst requiring substantial time and resources, has provided the robust clinical evidence necessary to support disc replacement technology adoption.
The process, whilst challenging, ultimately protects patients whilst facilitating the introduction of superior technologies that genuinely improve outcomes.
International Collaboration
Critical contributions have emerged from Sweden (Fernström's visionary concept), Germany (Büttner-Janz's engineering brilliance), France (Marnay-Bertagnoli's ball-and-socket design), and the United States (FDA regulatory framework).
This global collaboration continues to drive innovation, with researchers and clinicians worldwide sharing knowledge, clinical experience, and technological insights that benefit patients regardless of geographic boundaries.
A Legacy of InnovationAnd Hope
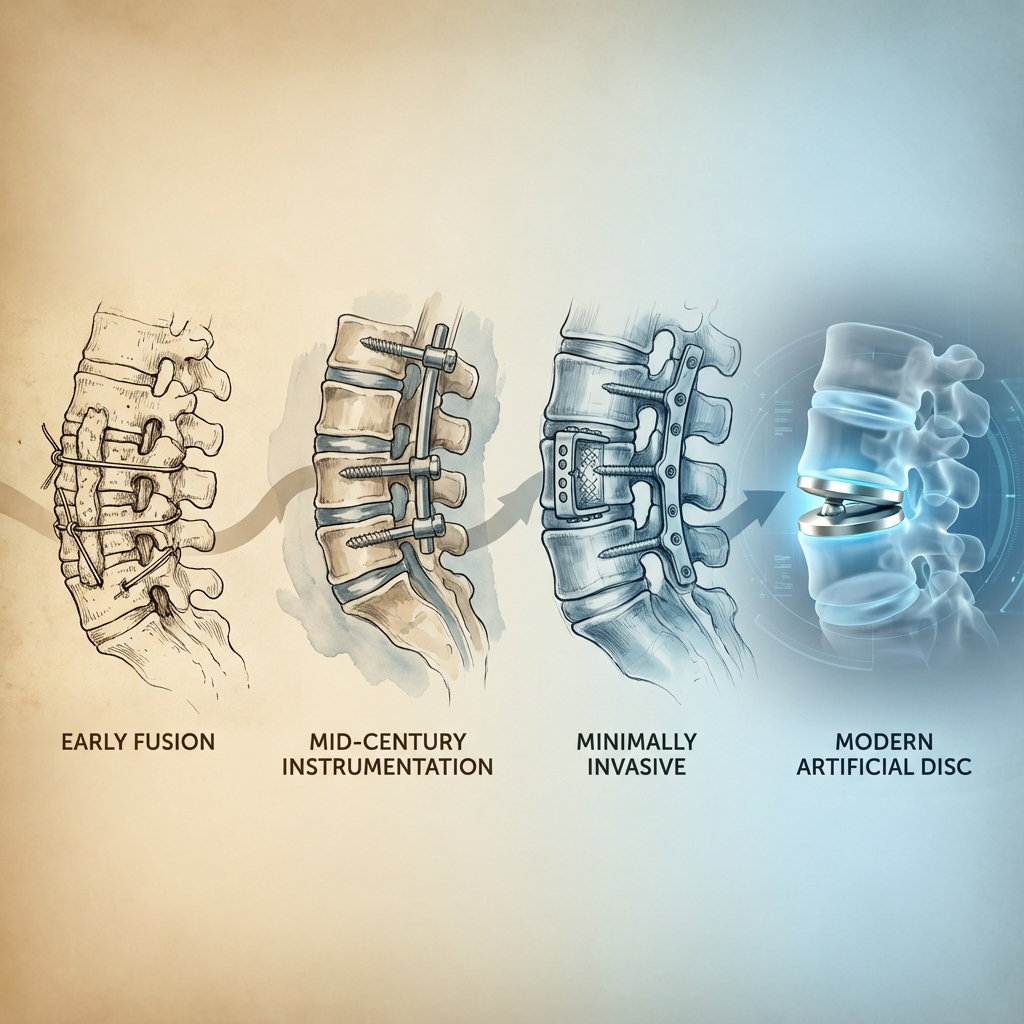
The extraordinary history of lumbar disc replacement spans more than six remarkable decades, evolving from Fernström's revolutionary but ultimately flawed steel spheres to today's sophisticated motion-preserving technologies that offer new hope to millions suffering from chronic back pain.
This incredible journey illustrates the profound complexity of medical device innovation, requiring decades of persistent research, extensive clinical experience, and continuous iterative refinement to achieve meaningful clinical success.
From Fernström's visionary concept through Büttner-Janz's engineering brilliance to contemporary biomimetic designs, each generation of pioneers has contributed invaluable knowledge to understanding spinal biomechanics and the exacting requirements for successful motion preservation.
Key Historical Achievements
Motion Preservation Validated
Successful maintenance of natural lumbar mobility throughout decades of clinical follow-up, validating Fernström's original vision whilst demonstrating superiority of modern engineering approaches.
Adjacent Segment Protection
Compelling evidence of more than 50% reduction in adjacent level problems compared to fusion surgery, confirming theoretical advantages.
Safety Validation
Acceptable complication profiles with predictable failure modes, established through 15,000+ devices implanted prior to FDA approval.
Global Adoption
Successful implementation across diverse healthcare systems worldwide, demonstrating universal applicability of motion-preserving principles.
Australian Contribution
The regulatory experience in Australia demonstrates the critical importance of evidence-based policy development whilst acknowledging the delicate balance between medical innovation and patient safety. The TGA's reclassification efforts reflect evolving understanding of device complexity and enhanced patient safety requirements.
Dr Aliashkevich's extensive Australian experience since 2012 exemplifies the successful clinical application of these revolutionary technologies, with hundreds of patients benefiting from motion-preserving surgery combined with comprehensive multidisciplinary care.
Future Horizons
Emerging Technologies
The next generation of lumbar disc replacement technology promises even more sophisticated solutions, building upon decades of accumulated knowledge and engineering refinement.
The Future of Motion Preservation
Next-generation technologies continue the legacy of innovation
Enduring Legacy and Future Promise
The story of lumbar disc replacement demonstrates that meaningful medical progress requires unwavering vision, persistent effort, and the courage to challenge established paradigms whilst respecting the crucial lessons learned through both triumph and disappointment.
The transformation from Fernström's simple spheres to today's sophisticated biomimetic devices represents one of medicine's most remarkable technological achievements, fundamentally improving the lives of patients worldwide whilst establishing motion preservation as a cornerstone of modern spine surgery.
The legacy continues to unfold, driven by the same spirit of innovation and dedication to patient welfare that motivated the earliest pioneers over six decades ago. Their collective vision of preserving human mobility whilst eliminating pain has become clinical reality, offering hope to future generations.
Epilogue: Honouring the Pioneers
Their Vision Made Motion Preservation Possible
This comprehensive history honours the extraordinary contributions of visionary surgeons, innovative engineers, dedicated researchers, and courageous patients who advanced the field of lumbar disc replacement from revolutionary concept to established clinical practice.
The successful development of lumbar arthroplasty demonstrates that medical innovation requires patience, humility to learn from failures, courage to persist through setbacks, and unwavering commitment to patient safety and clinical standards.