Cervical Disc Replacement History Technological Progress
Comprehensive history of cervical disc replacement technology from early concepts through modern TGA-approved implants. Understanding the evolution of motion-preserving technology demonstrates the scientific foundation and proven track record of cervical arthroplasty.
Early Concepts
Foundation Years
1950s
Pioneering work in the 1950s establishing the theoretical foundation for artificial disc replacement and motion preservation in spine surgery.
Clinical Introduction
Modern Era Begins
2007
Introduction of clinically proven cervical disc replacement systems with extensive clinical data and regulatory approval for widespread use.
Advanced Technology
Current Standards
2024
State-of-the-art cervical disc replacement with improved materials, design features, and clinical outcomes representing the latest in motion-preserving technology.
The Foundational EraEstablishing the Surgical Gateway
The story of cervical disc replacement begins not with artificial discs, but with the revolutionary development of anterior cervical spine surgery. This foundational work established the surgical gateway through which all subsequent motion-preserving innovations would pass.

Pioneers of Anterior Cervical Surgery
Anterolateral Cervical Disc Removal & Interbody Fusion
Johns Hopkins Hospital, Baltimore
- Seminal 1955 paper: "Anterolateral cervical disc removal and interbody fusion for cervical disc syndrome"
- Initial treatment of 8 patients with revolutionary anterior approach
- By 1962: 55 patients treated with remarkably consistent outcomes
- Established ACDF as gold standard for cervical disc pathology
Clinical Impact: Revolutionary paradigm shift from posterior methods—anterior access provided direct visualisation of pathological disc material, mechanical stability through bone fusion, and a reproducible technique adopted worldwide.
The Paradox of Early Success
The immediate success of early fusion procedures created an interesting paradox in spine surgery. Whilst validating the anterior approach, it also highlighted potential limitations that would drive future innovation.
Immediate Success
Excellent short- and medium-term clinical outcomes validated the anterior approach as revolutionary treatment.
Theoretical Concerns
Early observers including Dr William Scoville questioned whether fusion might accelerate adjacent segment degeneration.
Foundation Established
Surgical access proven effective and techniques refined, but the ideal motion-preserving solution remained elusive.
Stage Set
The demonstrated limitations of fusion set the stage for the next revolution in cervical spine surgery.
A Dual Legacy
This era established the foundation for all future cervical spine innovations: the surgical access was proven effective, the techniques were sufficiently refined and reproducible, but the ideal solution—preserving motion whilst addressing pathology—remained elusive. The stage was set for the next revolution.
Fernström's VisionThe Elegant Simplicity of Early Failure
Dr Ulf Fernström of Uddevalla, Sweden, deserves recognition as the true father of spinal arthroplasty. His revolutionary vision extended far beyond the conventional thinking of his era, anticipating concepts that would not fully mature for another four decades.
The concept captured the imagination of the spine surgery community and briefly offered hope for a truly superior alternative to fusion. Initially, Fernström reported encouraging results, claiming clinical outcomes comparable to fusion procedures whilst preserving motion. This early optimism proved premature.
Clinical Programme (1960s)
Published in 1966: "Arthroplasty with intracorporal endoprosthesis in the herniated disc and in the painful disc"
The Revolutionary Concept
Fernström's approach was elegantly simple: replace the degenerated disc with a solid stainless-steel sphere. Working with the Swedish Ball Bearing Factory, he adapted standard industrial ball bearings for spinal use.
The Reality of Biomechanical Failure
The Fernström Ball era ended in profound disappointment. The devices suffered from fundamental design flaws that reflected the limited understanding of spinal biomechanics available at the time.
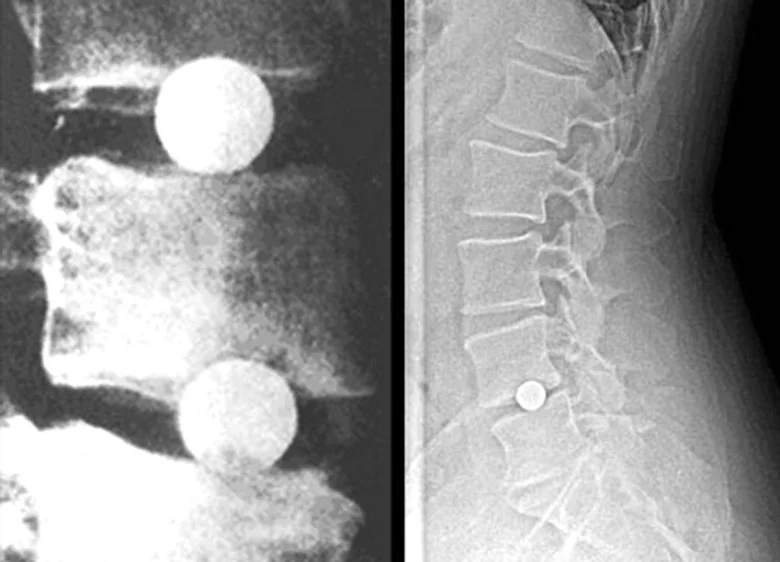
Subsidence & Material Incompatibility
Steel spheres eroded into vertebral endplates due to excessive contact pressures.
Technical Analysis
Mechanical property mismatch: steel modulus 200 GPa versus bone modulus 7-20 GPa created stress concentrations leading to progressive bone destruction.
Long-term complications: Extended follow-up revealed that 74% of patients developed moderate disc space narrowing due to subsidence, with many requiring revision surgery. By the 1970s, the combination of mechanical failures and poor outcomes led to abandonment of the procedure.
The Renaissance PeriodRenewed Interest and Innovation
The 1980s witnessed renewed interest in spinal arthroplasty, driven primarily by successful development of lumbar disc prostheses in Europe. As lumbar technology matured, attention naturally turned to adapting these concepts for the unique requirements of the cervical spine.
The Bristol Revolution
The modern era of cervical disc replacement began at Frenchay Hospital in Bristol, United Kingdom, where the Department of Medical Engineering developed a revolutionary two-piece articulating design.
Key Collaborators
- Dr Brian Cummins — Consultant Neurosurgeon
- Mr Steven Gill — Later Honorary Chair, University of Bristol
- James Robertson — Neurosurgical colleague
Two-piece articulating construction
Superior ball and inferior socket components that articulate naturally, allowing physiological motion
Secure anterior fixation
Anchoring screws designed to prevent migration—directly addressing a major Fernström Ball failure mode
Controlled motion patterns
Engineering principles derived from successful hip and knee arthroplasty experience
Improved biomaterials
Advanced stainless steel alloys with better biocompatibility than earlier devices
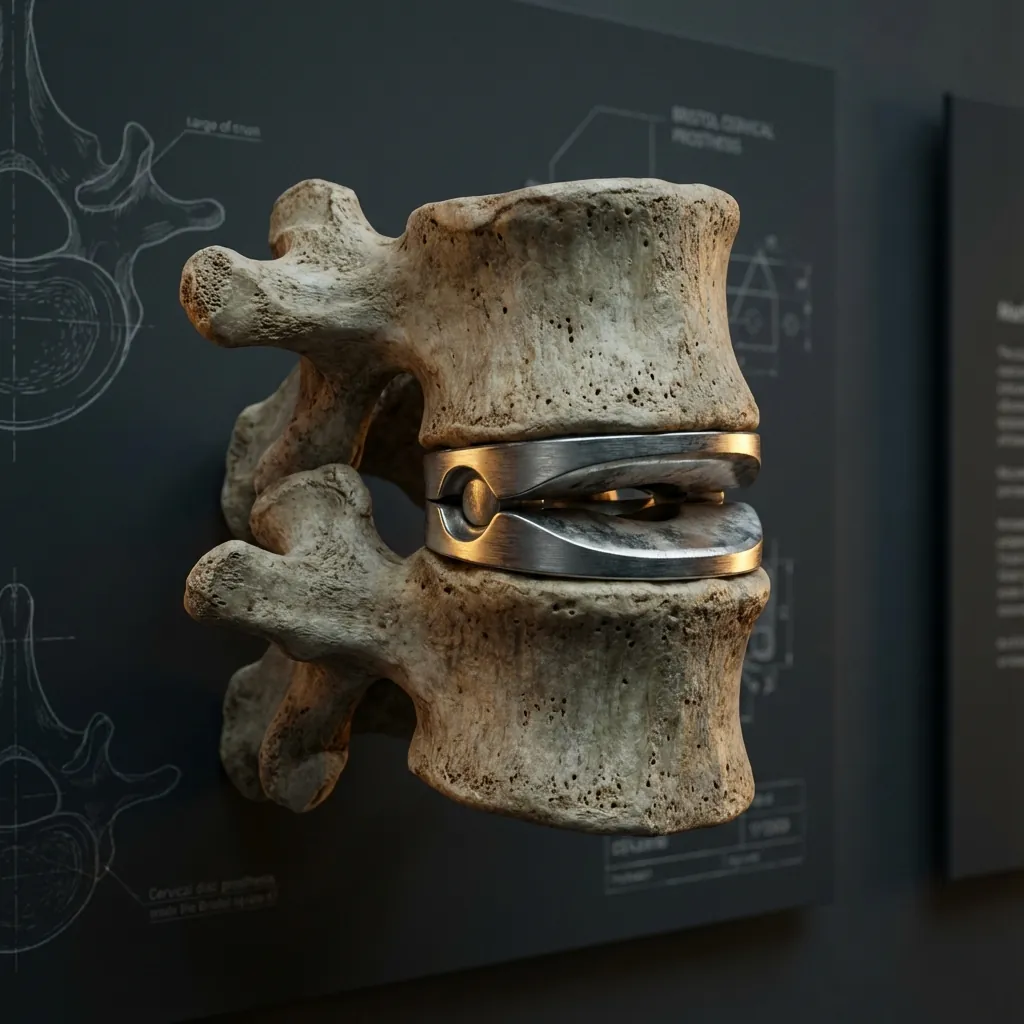
The Frenchay Evolution: From Failure to Success
Mr Steven Gill recognised the Bristol device's limitations and undertook comprehensive redesign efforts. Rather than abandoning the motion-preservation concept, Gill systematically addressed each primary failure mode whilst preserving the fundamental innovation.
Critical Milestones
Cummins-Bristol Joint
Dr Brian Cummins and hospital engineers at Frenchay Hospital, Bristol, create the first sophisticated articulating cervical disc prosthesis.
Clinical Significance
Quantum leap from simple Fernström Ball design with two-piece articulating construction.
Landmark 2004 Results
The multinational trial demonstrated significantly greater improvement in neck disability index scores at six weeks post-operation in the arthroplasty group, along with shorter operating times and reduced intraoperative blood loss. This landmark research provided robust Level I evidence of cervical arthroplasty's clinical efficacy.
The PRESTIGE LegacyFrom Frenchay to FDA Approval
Recognising the commercial potential of Gill's successful design, Medtronic acquired the technology and further refined it as the PRESTIGE® Cervical Disc System—transitioning academic innovation into global commercial development.

Strategic Acquisition
The acquisition provided resources necessary for extensive additional development, manufacturing scaling, and regulatory submission across multiple jurisdictions.
First FDA-approved cervical disc
Materials Advancement
Evolution from stainless steel to titanium-ceramic composites offering superior biocompatibility and wear resistance
Profile Optimisation
Further reduction to minimise soft tissue irritation and dysphagia risk
Manufacturing Quality
Industrial-scale production with consistent quality control standards
Clinical Validation
FDA Investigational Device Exemption studies with rigorous prospective design
FDA Approval Clinical Validation
The FDA approval was based on rigorous clinical trials comparing outcomes with ACDF, demonstrating superior performance across multiple clinical measures.
10-Year Follow-Up Data
Long-term follow-up data extending to ten years confirmed the durability of PRESTIGE benefits, establishing it as a proven alternative to fusion surgery.
Watershed Moment
The July 2007 FDA approval of the PRESTIGE ST marked a watershed moment for motion-preserving cervical surgery. Most importantly, reoperation rates at both index and adjacent levels were substantially lower with arthroplasty—validating the motion-preservation hypothesis that began with Fernström's vision four decades earlier.
Bryan's Biomimetic RevolutionThe Neurosurgeon-Inventor
While British engineers refined ball-and-socket designs, American neurosurgeon Dr Vincent Bryan developed a fundamentally different approach to cervical disc replacement—combining extensive clinical expertise with entrepreneurial vision.
Dr Vincent Bryan
Neurosurgeon & Inventor
Based in Seattle, Dr Bryan's background as a practicing neurosurgeon with Neurosurgery Northwest from 1975 to 1996 provided intimate understanding of cervical pathology and the practical limitations of existing treatments.
1992: Dr Bryan designed the Bryan Cervical Disc, representing several paradigm shifts in artificial disc technology.
International Clinical Development
The first Bryan disc was implanted in Belgium in 2000 by Professor Jan Goffin at the University Hospital Leuven, marking the beginning of European clinical experience.
FDA IDE Development Program
- • Prospective design eliminating selection bias
- • Randomised comparison with ACDF standard of care
- • Multiple centres ensuring diverse populations
- • Extended follow-up monitoring beyond early period
FDA Approval
Paradigm-Shifting Innovations
Biomimetic Design
Unique polyurethane sheath surrounding the nucleus, filled with saline
Technical Innovation
Unprecedented understanding of natural joint mechanics—the first attempt to replicate the biochemical environment of a natural disc. The saline-filled system created a closed-system bearing surface more akin to natural joints.
Outstanding 10-Year Results
Commercial Journey & Legacy
Originally developed through Dr Bryan's company and eventually acquired by Medtronic, the Bryan disc's biomimetic approach influenced subsequent device development—particularly the emphasis on natural motion patterns, biocompatibility, and closed-system wear management. The 10-year results validated this innovative philosophy and established the Bryan disc as a benchmark for cervical arthroplasty success.
ProDisc DevelopmentThe Ball-and-Socket Philosophy
The development of cervical disc replacement flourished in France and Germany under the collaborative guidance of Dr Thierry Marnay and Dr Rudolf Bertagnoli—representing a natural evolution from successful lumbar arthroplasty principles.
Design Philosophy
This philosophical difference—between biomimetic (Bryan) and biomechanical (ProDisc) design approaches—represented genuine innovation in competing conceptual frameworks, both achieving successful clinical outcomes.

Design Characteristics
Materials Selection
Cobalt-chromium alloy endplates providing superior wear resistance derived from decades of hip and knee arthroplasty experience
Bearing Surface
Ultra-high-molecular-weight polyethylene (UHMWPE) offering proven long-term durability from extensive orthopaedic applications
Articulation Design
Ball-and-socket configuration with established track record in weight-bearing joints, featuring constrained motion for stability
Fixation Method
Keel fixation mechanism adapted from successful lumbar experience, distributing forces across the endplate surface
7-Year Clinical Results
Clinical results demonstrated equivalent or superior efficacy to ACDF with motion preservation benefits and significantly lower reoperation rates—establishing the ball-and-socket design as a proven approach to cervical arthroplasty.
Commercial Evolution
FDA Approval
December 17, 2007 — Second cervical disc approved by FDA
The technology transitioned through Spine Solutions → Synthes → DePuy-Synthes (Johnson & Johnson) → Centinel Spine (2017)—reflecting the substantial investment required for global commercial development.
Orthopaedic Heritage
The ProDisc-C's design philosophy paralleled proven principles of hip and knee arthroplasty, providing surgeons with familiar concepts adapted for spinal application. The consistency of results across multiple studies established the ball-and-socket design as a validated approach—demonstrating that different design philosophies could both achieve excellent clinical outcomes.
The Australian ExperiencePolicy Evolution and Clinical Adoption
Australian spine surgeons were among the early international adopters of cervical arthroplasty technology, contributing to growing evidence and demonstrating the complex relationship between medical innovation and healthcare policy.
Medicare Policy Journey
MSAC reverses position, recognising cervical arthroplasty as more effective than ACDF based on "overall success" measures at 24 months.

Early Clinical Leadership
Australian spine surgeons were among the early international adopters of cervical arthroplasty technology, reflecting the progressive nature of Australian medicine and strong connections with international spine surgery communities.
Many Australian surgeons utilise cervical disc replacement and achieve excellent results with hundreds of patients.
- Single-level procedures
- Multilevel procedures
- Hybrid procedures (arthroplasty + fusion)
- Contributing to broader evidence base
Note: Multi-level procedures are not currently covered under Medicare, reflecting the evidence base available at policy determination.
Contemporary TGA-Approved Implants
Recent developments have expanded options available to Australian surgeons. In March 2025, the MOVE-C artificial disc prosthesis by NGMedical GmbH received TGA approval, bringing advanced viscoelastic technology designed to more closely replicate natural disc mechanics. The expanding portfolio of TGA-approved devices provides Australian surgeons with evidence-based alternatives to fusion surgery.
The Modern EraTechnological Sophistication
The period from 2007 to 2024 witnessed systematic FDA approval of multiple cervical disc prostheses, each representing incremental advances in design philosophy, biomaterial science, and clinical validation.

FDA Approval Timeline
PRESTIGE ST
Medtronic
First FDA-approved cervical disc
ProDisc-C
Centinel Spine
Ball-and-socket design based on lumbar experience
Bryan
Medtronic
Biomimetic polyurethane design
NuVasive PCM
NuVasive
Metal-on-polyethylene with porous coating
Mobi-C (Single)
Zimmer Biomet
Streamlined design from lumbar experience
Mobi-C (Two-Level)
Zimmer Biomet
First FDA approval for two-level arthroplasty
M6-C
Orthofix (discontinued 2023)
Viscoelastic technology with fiber annulus
Simplify
Simplify Medical
PEEK endplates reducing MRI artifact
Baguera-C
Spineart
High-density polyethylene nucleus with elastic deformation
The superiority effect was more pronounced with two-level procedures, likely because motion preservation provided greater advantage in preserving global cervical spine kinematics.
Design Philosophy Evolution
Metal-on-Metal
PRESTIGE series
Emphasises durability and wear resistance with titanium-ceramic composites
Metal-on-Polyethylene
ProDisc-C, Mobi-C
Proven bearing surface technology from orthopaedic arthroplasty
Advanced Polymers
Bryan, M6-C
Biomimetic replication of natural disc function
Emerging Technologies
Simplify
PEEK endplates with ceramic nuclei for MRI compatibility
Maturation of Motion-Preserving Technology
This expansion reflects the maturation of cervical arthroplasty as a mainstream treatment option with multiple proven approaches. Different approved devices embody fundamentally different design philosophies—metal-on-metal, metal-on-polyethylene, advanced polymers, and emerging technologies—each achieving excellent clinical outcomes through different biomechanical strategies.
Evidence-Based OutcomesLevel I Clinical Validation
The modern era of cervical arthroplasty is distinguished by extensive high-quality clinical evidence from prospective, randomised controlled trials—representing one of the most rigorous evaluations of any spinal surgical innovation in history.
2024 Comprehensive Review
A comprehensive systematic review and meta-analysis published in 2024 analysed 31 studies including 17 randomised controlled trials, demonstrating consistent findings across multiple devices and surgical teams.
Key Findings
Superior overall success rates
Clinical OutcomesCervical arthroplasty demonstrated comparable or superior clinical success to ACDF across multiple outcome measures, with effect sizes becoming more pronounced with longer follow-up.
Cadaveric studies demonstrated that cervical fusion significantly increases intradiscal pressure at adjacent levels, while arthroplasty maintains normal stress distribution patterns.
Evidence Base Summary
This evidence base provides confidence in both the safety and efficacy of cervical arthroplasty when appropriately indicated.
Lessons From HistoryPrinciples for Continued Success
The remarkable journey of cervical disc replacement—spanning more than a century of surgical development—offers profound lessons that continue to guide innovation toward even better solutions for cervical spine pathology.

Key Achievements
Critical Lessons
Biomechanical Understanding
The evolution from Fernström's simple ball bearings to today's sophisticated devices illustrates the fundamental importance of understanding spinal biomechanics.
This comprehensive history honours the contributions of countless surgeons, engineers, researchers, and patients who advanced cervical disc replacement from visionary concept to clinical reality.
A Remarkable Century of Progress
The successful development of cervical arthroplasty demonstrates that medical innovation requires patience, humility to learn from failures, courage to persist through setbacks, and unwavering commitment to patient safety and clinical standards.
The transformation from Fernström's simple spheres to today's sophisticated biomimetic devices represents one of medicine's most remarkable technological achievements—inspiring continued innovation in motion-preserving spinal surgery for patient the decades ahead.