
Lumbar Surgical Technique Surgical Standards
Advanced lumbar disc replacement surgical techniques featuring anterior approach methods with multidisciplinary vascular collaboration, microsurgical standards, and optimal implant positioning ensuring superior surgical outcomes and patient safety.
Vascular Approach
Multidisciplinary Team
Anterior
Advanced anterior surgical approach with vascular specialist collaboration ensuring safe access to lumbar disc space and optimal surgical outcomes for complex cases.
Microsurgical Technique
Advanced Methods
Standards
Advanced microsurgical techniques ensuring accurate implant positioning and optimal biomechanical function while minimizing tissue disruption and surgical trauma.
Invasive Approach
Reduced Recovery Time
Minimally
Minimally invasive surgical approach with reduced operative time, minimal complications, and accelerated recovery compared to traditional posterior surgical approaches.
Why Lumbar Surgery Is DifferentApproach Considerations
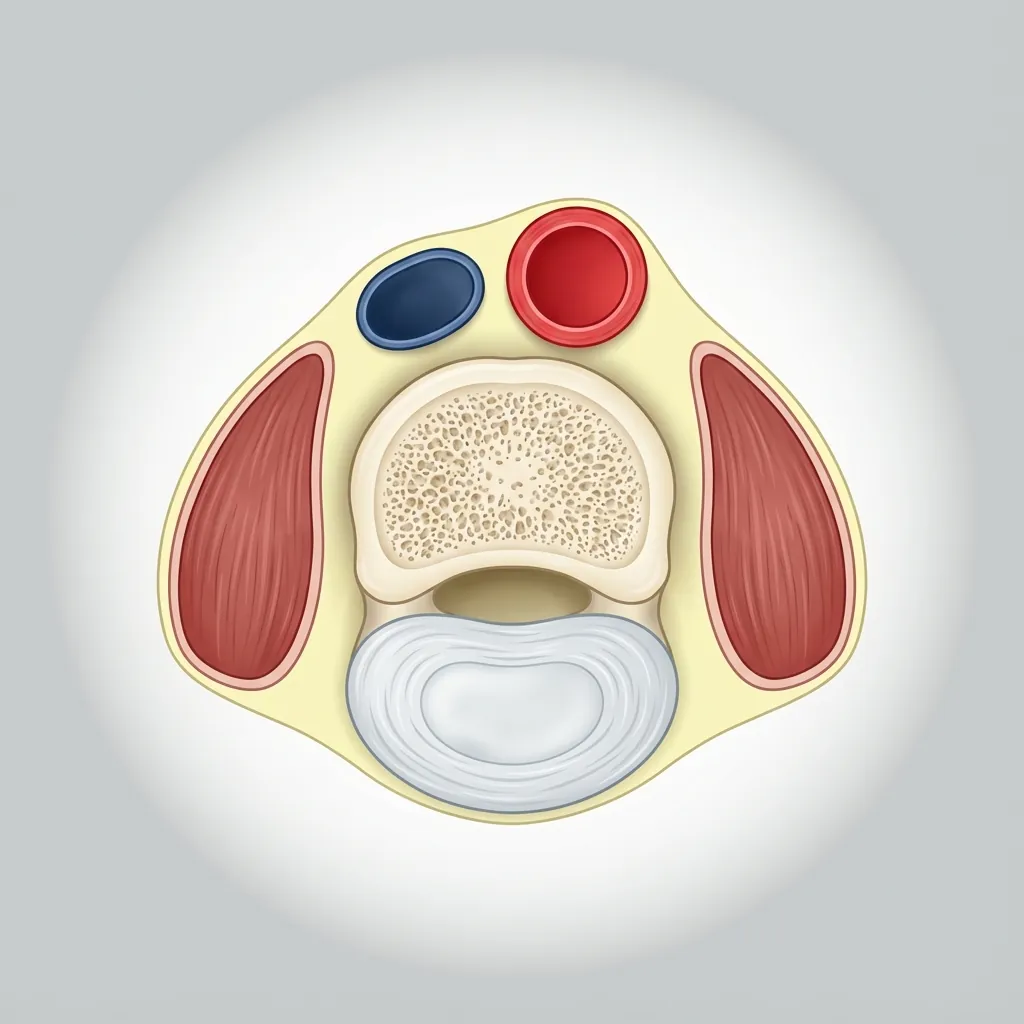
Lumbar disc replacement surgery is fundamentally different from cervical because the lumbar spine is under much greater axial load and has significant vascular structures nearby.
Clinical Relevance
The anterior approach is the gold standard for lumbar disc replacement because it provides direct access to the disc space without disturbing the posterior spinal elements, muscles, or neural structures.
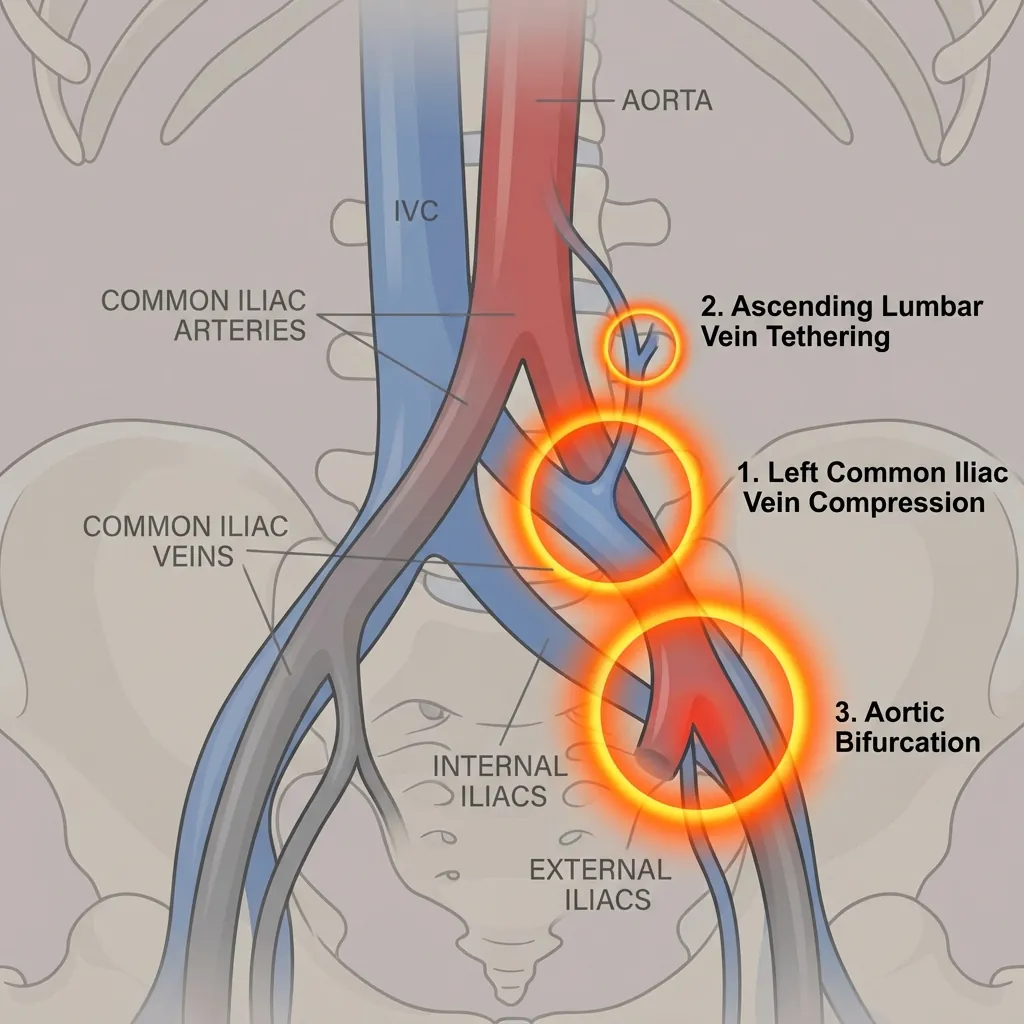
Vascular Surgeon CollaborationThe Essential Team Member
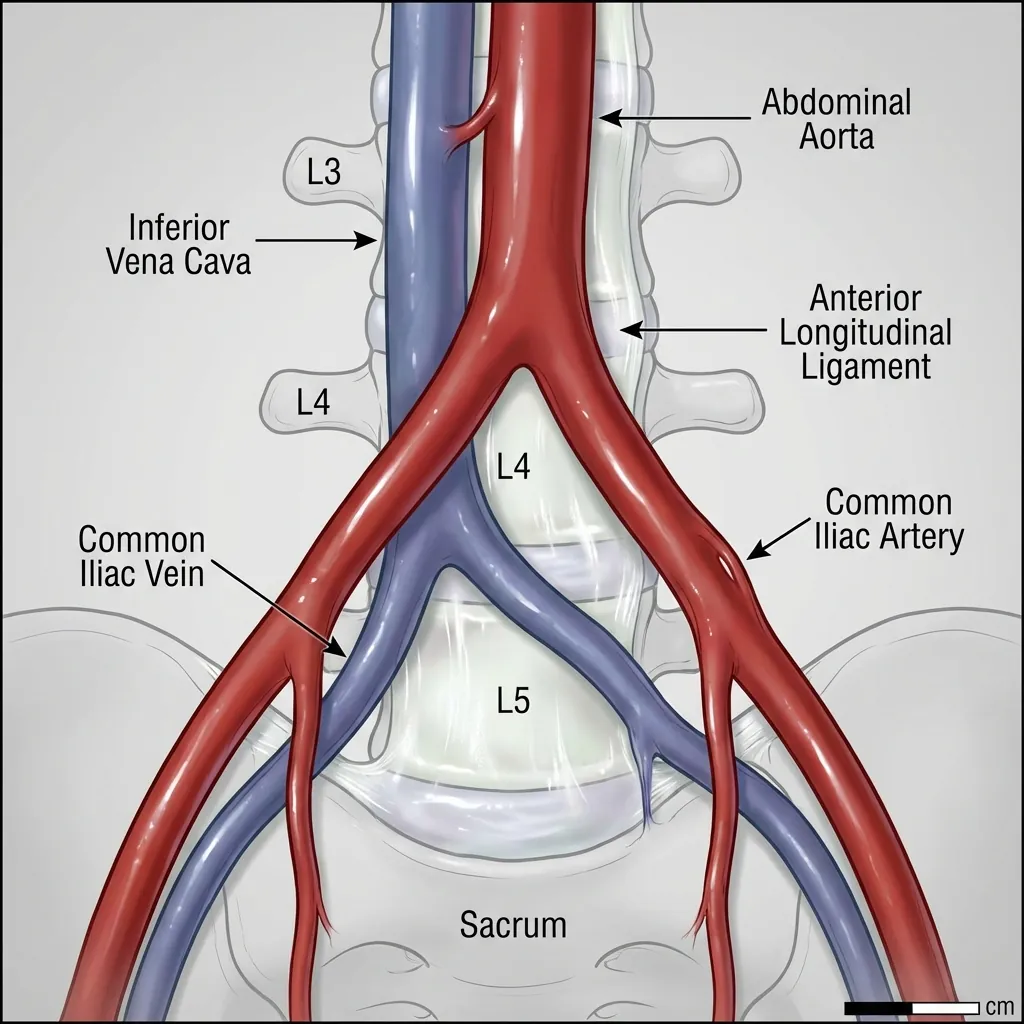
This is the single biggest difference between cervical and lumbar disc replacement surgery. In lumbar anterior surgery, major vessels (aorta, inferior vena cava, iliac vessels) are directly in the surgical field.
Why This Matters
In cervical surgery, vascular complications are rare (0.5–1.5%) and usually manageable on the spot. In lumbar anterior surgery, vascular complications are more common (1–3%) and potentially catastrophic if not properly managed. This is why experienced vascular surgeon collaboration is essential—not just available, but present and planning.
Risk Stratification Categories
Low Risk
Normal vessel anatomy, no atherosclerosis, good vessel space for access
Intraoperative Vascular Surgeon Role
Vessel Retraction Technique
Why gentle retraction matters: Aggressive compression causes thrombosis (clotting), ischaemia damages the vessel, and can cause acute vessel occlusion intraoperatively or thrombosis postoperatively. Proper gentle technique prevents this.
Anterior Lumbar ApproachStep-by-Step Technique
The anterior approach requires layer-by-layer abdominal access with meticulous attention to positioning and vascular structures.
Patient Positioning (Anterior Approach)
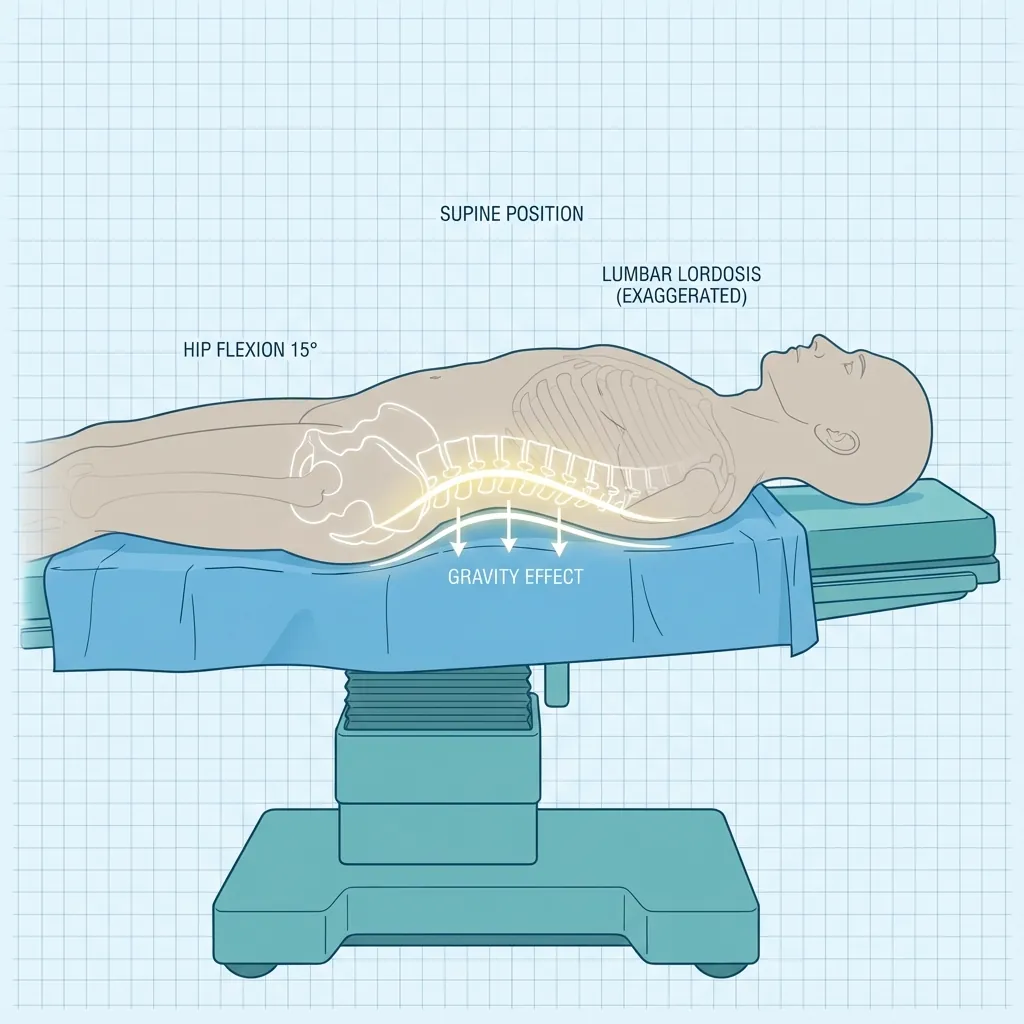
Different from cervical—lumbar anterior requires supine positioning:
Patient supine (lying on back) on OR table
Arms extended on armboards (out of surgical field)
Legs straight or slight flexion (depends on approach level)
No padding under lumbar spine (want gravity to help open disc space)
Fluoroscopy positioned laterally (for side X-rays to identify level)
Why this positioning matters:
Supine allows vascular surgeon easy access to vessels
No muscle compression (patient gravity assists exposure)
Good fluoroscopy angles for level confirmation
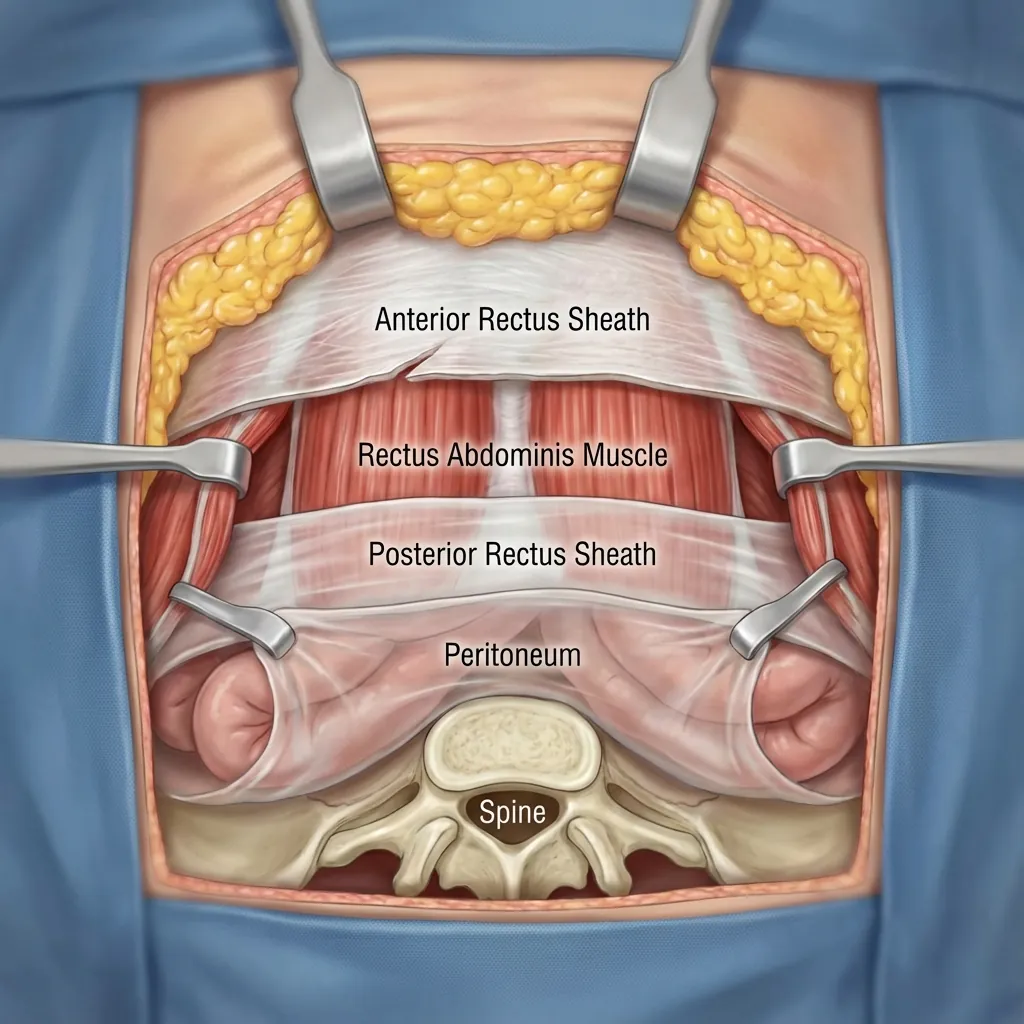
Anterior Incision and Abdominal Access
Layer-by-layer abdominal access is required. Each layer must be carefully navigated to reach the spine while protecting vital structures.
Vascular Identification (Critical Step)
This is THE critical step for anterior lumbar approach:
Identification:
Lateral Dissection (Opening the Vascular Corridor)
1. Left lateral dissection
Peritoneum and left-sided structures reflected left. Aorta and left iliac artery exposed. Aorta identified and palpated (confirms anatomy matches imaging).
2. Right lateral dissection
Peritoneum and right-sided structures reflected right. IVC and right iliac vein exposed. IVC identified and palpated.
3. Anterior dissection (carefully)
Anterior adventitia (connective tissue) of vessels carefully dissected. Lymphatic tissue and small vessels ligated with care. Creates space to access anterior vertebral bodies.
Retraction Setup
Vascular surgeon typically holds retraction or supervises retractors. Aorta and IVC gently retracted (never aggressively). Retraction pressure continuously monitored. Frequent release of retraction (every 10–15 minutes).
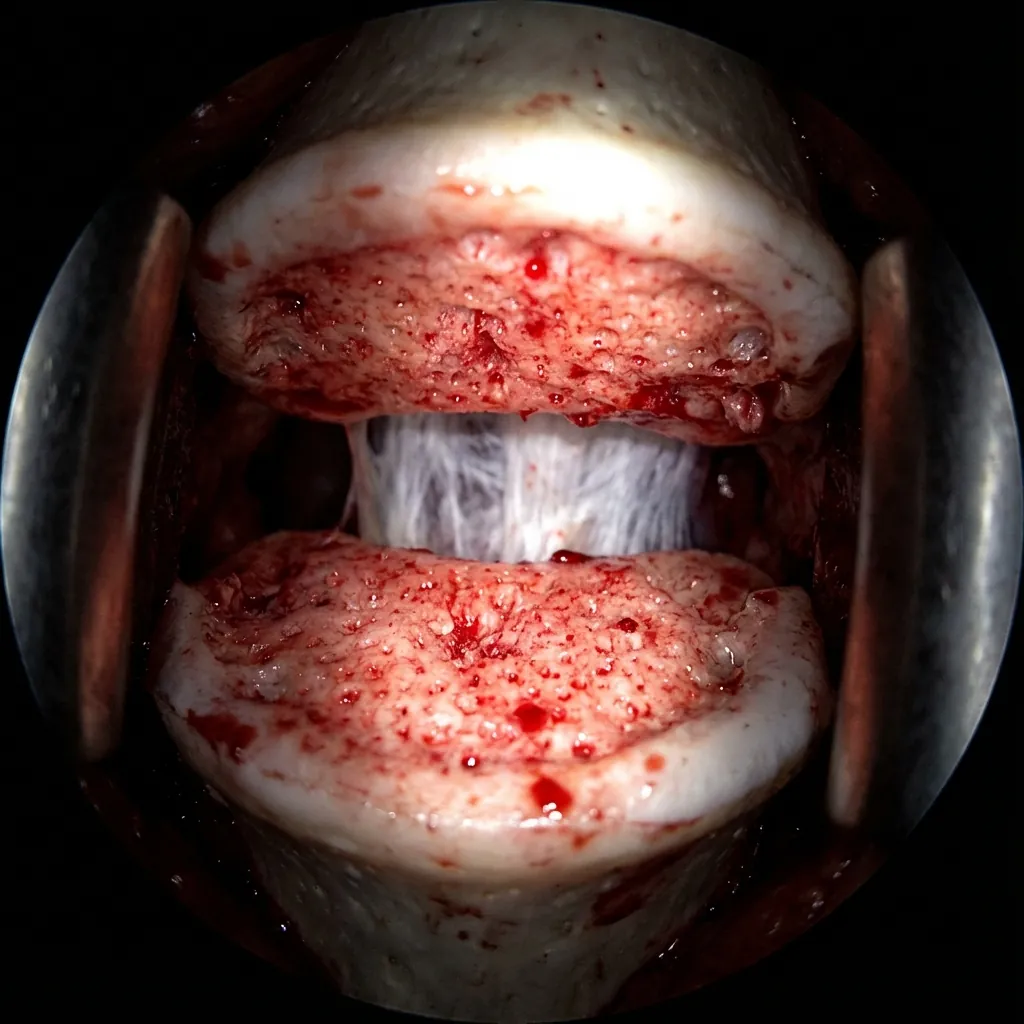
Discectomy & Endplate PreparationLumbar-Specific Technique
Lumbar discs bear significant axial load, so preparation is meticulous. Perfect endplate preparation is critical for implant success and long-term stability.
Access to Disc Space
Once vessels are controlled, the surgical level is identified:
Why Technique Matters in Lumbar
Cervical discs support light loads (head weight ~5–6 kg). Lumbar discs support heavy loads (torso weight 30–50 kg plus movements). This magnifies the importance of perfect endplate preparation.
Disc Space Height Restoration
Gradual disc space distraction is essential:
Distraction device places gentle upward pressure between vertebrae
Gradual increase over time (10–15 minutes for lumbar, longer than cervical)
Neuromonitoring confirms no nerve compression
Fluoroscopy shows increasing disc height
Foramen opening confirmed
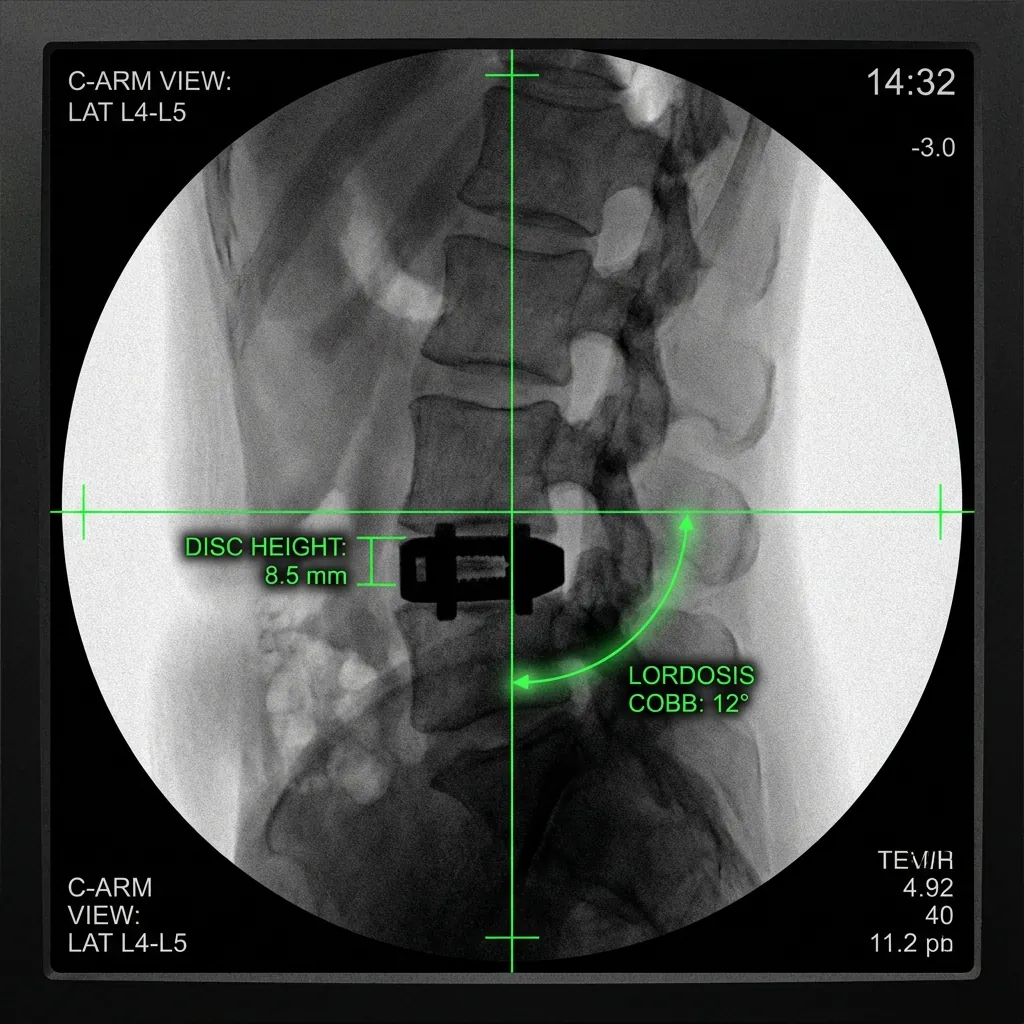
Target Height
Preoperative disc height measured from imaging
Restore to normal or slightly above
Typical lumbar disc height: 8–12mm depending on level
Slightly higher than preop compensates for implant compression
Implant Selection & PositioningStandards for Load-Bearing
Lumbar implant sizing is more complex than cervical due to load-bearing requirements. Perfect positioning is critical due to the high forces involved.
Lumbar Implant Sizing
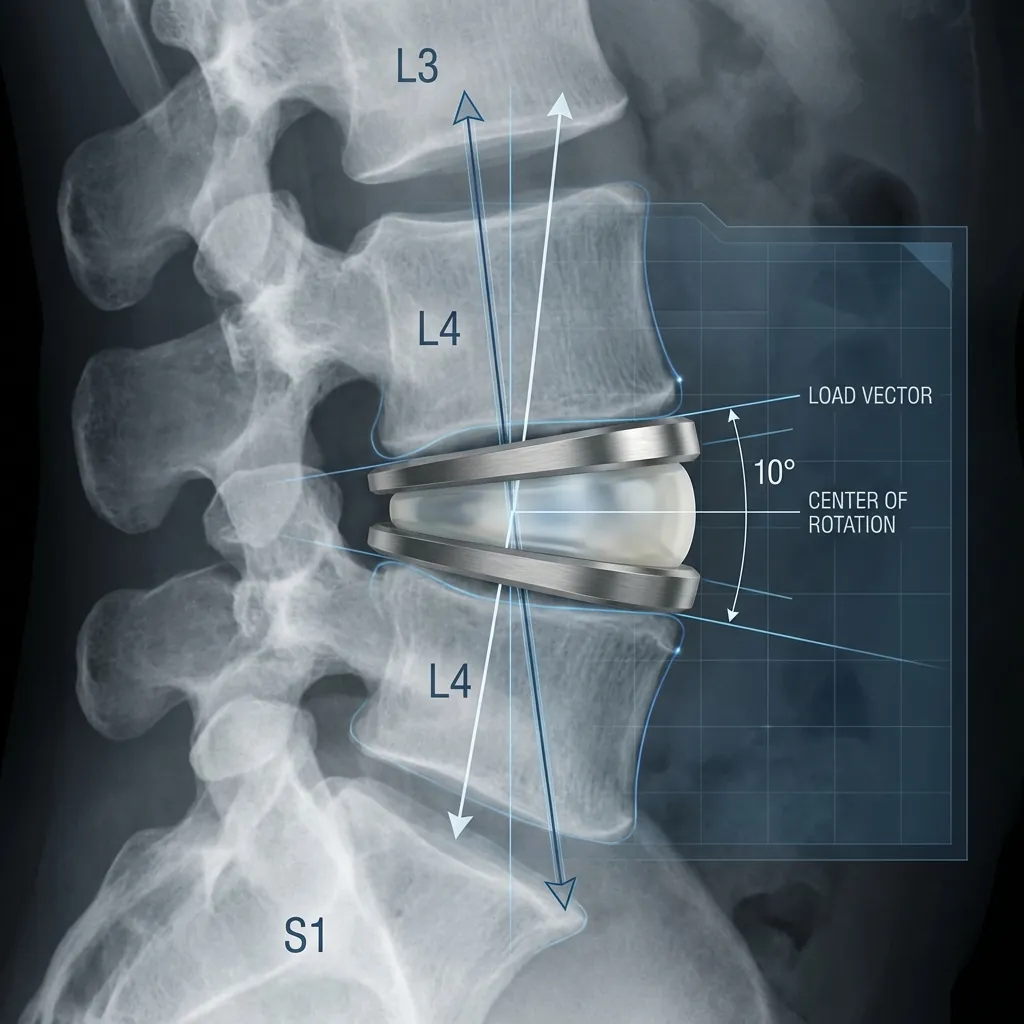
Sagittal Balance and Lordosis Restoration(THE Key Difference)
Why It Matters
Cervical spine is relatively light-loaded
Lumbar spine is weight-bearing for entire torso
Lumbar lordosis (forward curve) is essential for normal weight distribution, normal gait mechanics, prevention of adjacent-segment degeneration, and long-term spine health
Assessment
Implant Bearing Surface Options
Lumbar implants typically have more wear exposure than cervical (higher loads, longer lifespan). Because loads are higher and implants may be in situ 40+ years, bearing surface choice is more critical in lumbar than cervical.
Advantages
Proven long-term track record
Considerations
Theoretical wear concerns with higher lumbar loads
Midline Centering and Positioning
Perfect positioning is even more critical in lumbar due to load-bearing:
Medial-Lateral Centering (Left-Right)
Implant must be perfectly centred
Deviation causes asymmetric loading
Asymmetric loading → facet overload → facet pain, faster facet degeneration
Assessed by direct visualisation, fluoroscopy (AP view), measurement instruments
Anterior-Posterior Depth
Implant positioned to maximise endplate contact
Not too far anterior (compromises anterior support)
Not too far posterior (risks cord/nerve compression)
Optimal: Implant endplates in full contact with vertebral endplates
Lordotic Angle Orientation
If lordotic implant, must be oriented correctly
Anterior aspect positioned anteriorly (to create forward curve)
Incorrect orientation → kyphosis (backward curve) instead of lordosis
Confirmed by lateral fluoroscopy
Height Verification
Implant height restores disc space
Too-low height → incomplete decompression, insufficient lordosis
Too-high height → excessive distraction, ligament stress, myelopathy risk
Direct Visualisation
Microscope inspection of implant position, medial-lateral centering, endplate contact, foramen decompression
Fluoroscopic Verification
Lateral view: AP depth, lordotic angle, disc height restoration, segmental alignment. AP view: Medial-lateral centering, absence of lateral shift, symmetry. Oblique views: Foramen assessment, foraminal decompression confirmation.
Measuring Verification
Specialised instruments measure disc space height, confirm restoration to target height, assess biomechanical spacing.
Lumbar-Specific Consideration
Your surgeon should explain their specific bearing surface choice for your situation. Multiple verification methods confirm optimal positioning before closure.
Vascular ComplicationsAnterior Approach Risks
While rare, understanding how vascular injury is recognised and managed is important. Prevention is absolutely paramount.
Prevention: The Key Strategy
Careful preoperative assessment of vascular anatomy
Appropriate approach selection based on anatomy
Vascular surgeon involvement in planning and possibly surgery
Gentle dissection technique (not aggressive)
Frequent release of retraction (prevents ischaemia)
Clear team communication about vessel status
Vascular surgeon immediately available if problems occur
Key Point
Prevention of vascular injury is absolutely paramount. With careful preoperative assessment, appropriate approach selection, experienced vascular surgeon collaboration, and meticulous surgical technique, these complications are rare.
Visceral & Neurological ComplicationsPrevention and Management
Beyond vascular complications, the anterior and lateral approaches carry other specific risks. Prevention is key through experienced technique.
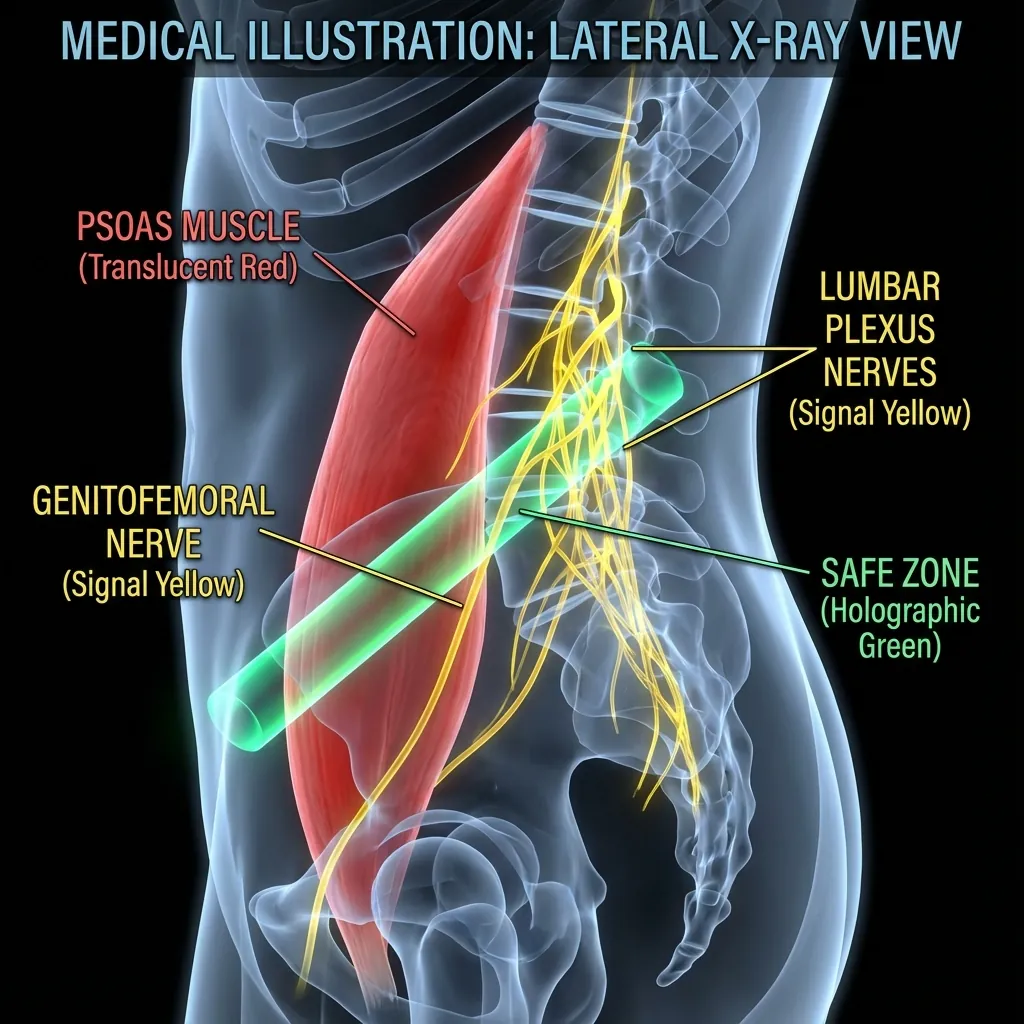
Prevention is key: Experienced anterior surgeon, careful technique, and meticulous attention to anatomical planes minimise these risks significantly.
Closure Technique & HaemostasisCritical for Lumbar
Lumbar approach causes more bleeding than cervical—meticulous haemostasis is essential. Proper layer-by-layer closure ensures optimal healing.
Achieving Complete Haemostasis
Identify Bleeding Sources
Muscular bleeders from dissection
Venous ooze from endplates
Bone ooze from vertebral bodies
In anterior approach: potential retroperitoneal vessels
Achieve Haemostasis
Electrocautery: Bipolar cautery near neural structures, monopolar on muscle
Topical haemostatic agents: Thrombin, haemostatic gauze, collagen
Bone wax: Applied to bone bleeding (endplates, vertebral bodies)
Suture ligation: For larger vessels
Final Inspection
Entire surgical field dry
No bleeding points
No haematoma accumulating
Surgical field clean and dry
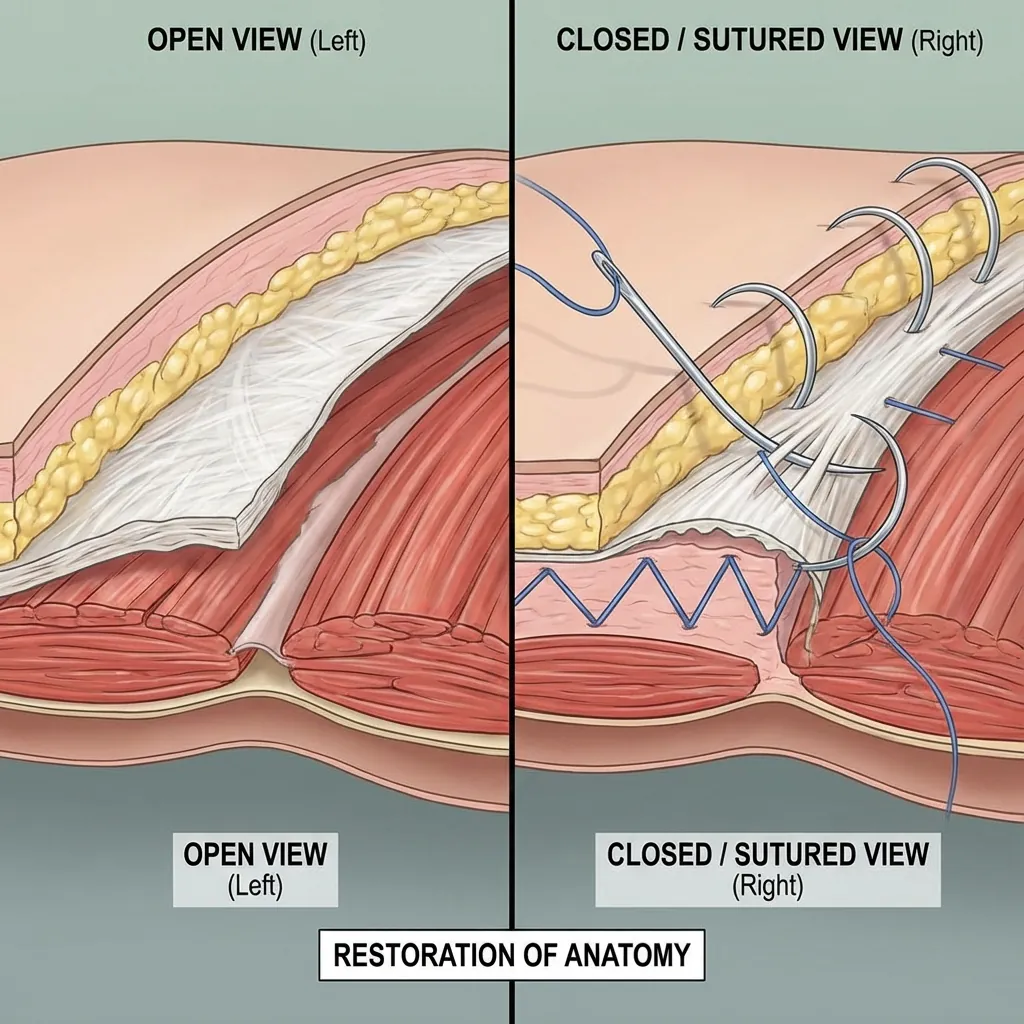
Anterior Approach Closure (Deep to Superficial)
Critical for Success
Meticulous haemostasis before closure and anatomical layer-by-layer closure technique are essential for preventing postoperative haematoma and ensuring optimal wound healing.
Quality AssuranceLumbar-Specific Metrics
Surgeon assesses key metrics before concluding surgery and ensures comprehensive documentation for quality and continuity of care.
Intraoperative Quality Metrics
Comprehensive Documentation
Comprehensive documentation ensures quality and continuity of care. All essential details including implant serial numbers, verification findings, and any complications are recorded for long-term patient management.
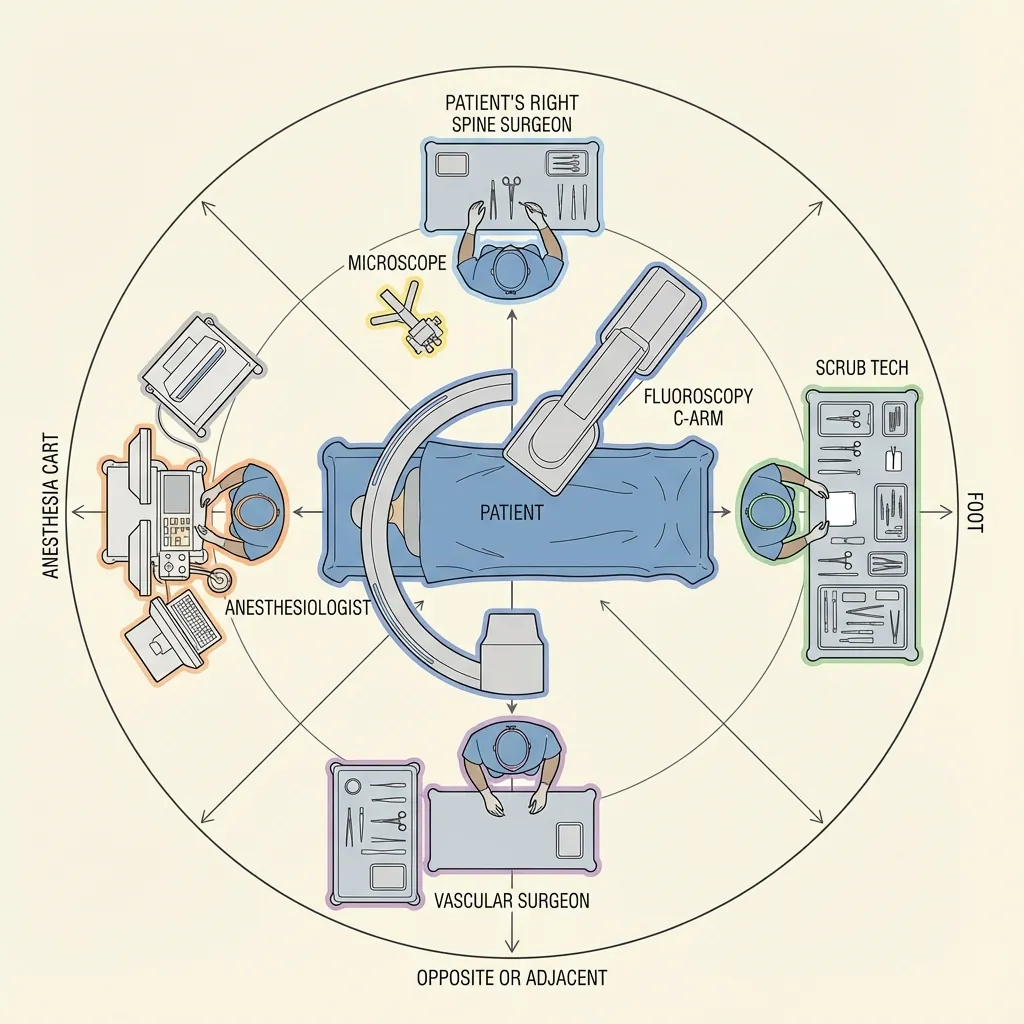
Multidisciplinary TeamLumbar-Specific Roles
Lumbar disc replacement requires a highly coordinated multidisciplinary team, with special emphasis on vascular surgeon collaboration for anterior approaches.
Preoperative Multidisciplinary Planning
Complex cases involve detailed planning:
Vascular surgery meeting: Review of imaging, discussion of approach feasibility, planning for vessel management
Anaesthesia consultation: Medical optimisation, positioning discussion, potential difficulty assessment
Neuromonitoring planning: Discussion of baseline concerns, anticipated monitoring needs
Team huddle: Everyone understands the plan and their role
Intraoperative Communication Protocol
Critical team coordination during surgery:
Neuromonitoring tech alerts surgeon to any baseline changes
Surgeon acknowledges and responds (reducing retraction, repositioning, etc.)
Anaesthesiologist informs team of haemodynamic status during vascular retraction
Vascular surgeon advises on retraction tolerances and vessel status
Surgical team coordinates all movements to avoid vessel compression or nerve trauma
All team members stay focused on shared goal of excellent surgical outcome
Team Cohesion
The success of lumbar disc replacement surgery depends not just on the spine surgeon's skill, but on the seamless coordination of the entire multidisciplinary team. Each member plays a critical role in ensuring patient safety and optimal outcomes.
Surgeon Expertise & Learning CurveLumbar-Specific Requirements
Successful lumbar disc replacement requires approach-specific skills. Surgeon experience and case volume dramatically affect complication rates and outcomes, especially for lateral approach.
Technical Skills Required (Lumbar-Specific)
Anterior Approach Skills
Abdominal anatomy knowledge
Vascular anatomy understanding and safe vessel handling
Retroperitoneal dissection experience
Fluoroscopic guidance capability
Implant sizing judgement for load-bearing context
Learning Curve
Critical Insight
Surgeon experience and case volume dramatically affect complication rates and outcomes, especially for lateral approach. The learning curve is significant, and patients should consider surgeon experience when selecting their surgical team.
Training and Certification: What to Look For
Fellowship training in spine surgery (1–2 years specialised training)
International training exposure (US, Europe, Asia techniques)
Specific approach training: Proctorship or mentorship in lumbar-specific approaches
Ongoing education: Regular courses and continuing education
Case volume: Minimum 50–100 of specific procedure for competency
Low complication rates: Published or verifiable complication data
Long-term outcomes tracking: Evidence of attention to patient outcomes
Surgical Standards in Lumbar Disc ReplacementThe Complete Picture
Lumbar disc replacement is a sophisticated, complex surgical procedure with anterior approach-specific techniques, requiring extensive expertise.
The Complexity and Sophistication of Lumbar Surgery
Lumbar disc replacement is more complex than cervical surgery because:
Vascular challenges demand specialised team collaboration and planning
Load-bearing biomechanics require precise implant selection and positioning
Sagittal balance considerations demand attention to long-term spinal health
Learning curves are steeper (especially lateral approach)
Complication spectrum is broader (vascular, visceral, neurological)
Surgical Quality Requires
Meticulous patient positioning and approach-specific setup
Careful anterior exposure with vascular surgeon collaboration (if anterior approach)
Precise discectomy and endplate preparation with load-bearing in mind
Accurate implant selection and positioning with lordosis restoration
Continuous neuromonitoring and safety vigilance
Methodical verification of decompression and implant placement
Careful, detailed closure with optimal haemostasis
Complication prevention through anticipation, experience, and team coordination
Comprehensive documentation and quality assurance
Your Surgeon's Responsibility
Your surgeon commits to:
Assess your specific anatomy and pathology
Select appropriate approach based on your situation
Execute surgery with technical proficiency and safety vigilance
Manage any complications that arise
Provide comprehensive education on findings and recovery
Facilitate optimal rehabilitation and return to function
Track long-term outcomes to ensure success
Understanding the Surgical Technique Helps You Appreciate
Why thorough preoperative assessment is necessary
Why vascular and neuromonitoring are critical (especially anterior approach)
Why your surgeon's experience and approach selection matter
Why different approaches exist and why one might be better than another for YOU
Why careful postoperative rehabilitation is important
Final Thoughts
Surgical quality in lumbar disc replacement—combining meticulous technique, continuous safety vigilance, multidisciplinary collaboration, and thoughtful decision-making—transforms preoperative planning into optimal surgical outcomes and long-term lumbar spine health.
Whether your surgeon chooses anterior, lateral, or posterior approach, the principles are the same: technique, safety, and respect for the complexity of the lumbar spine.