Cervical And Lumbar Disc Replacement Motion-Preserving Spine Surgery
Treatment of chronic neck or back pain shouldn't mean sacrificing mobility. Artificial Disc Replacement (ADR) preserves natural movement whilst addressing the underlying problem and offering a modern alternative to traditional fusion. Consult an internationally trained neurosurgeon specialising in advanced motion-preserving spine surgery, to discuss cutting-edge cervical and lumbar disc replacement procedures with multidisciplinary collaboration to achieve evidence-based outcomes, aiming to protect long-term spinal health.
Surgical Standards
International Training & Experience
30+ Years
Over 30 years of specialised experience in neurosurgery and spine surgery with international training from world-leading medical institutions. Continuously advancing motion-preserving techniques through ongoing research and professional development.
Successful Procedures
Minimally-invasive Surgeries
3000+
More than 3,000 spinal procedures performed with excellent outcomes. Expertise in arthroplasty, complex multi-level cases and minimally-invasive surgeries for optimal patient results.
Patient Satisfaction
Evidence-Based Outcomes
98%
98% patient satisfaction rate based on comprehensive outcome measures including pain reduction, functional improvement, and quality of life enhancement. Validated through long-term follow-up studies.

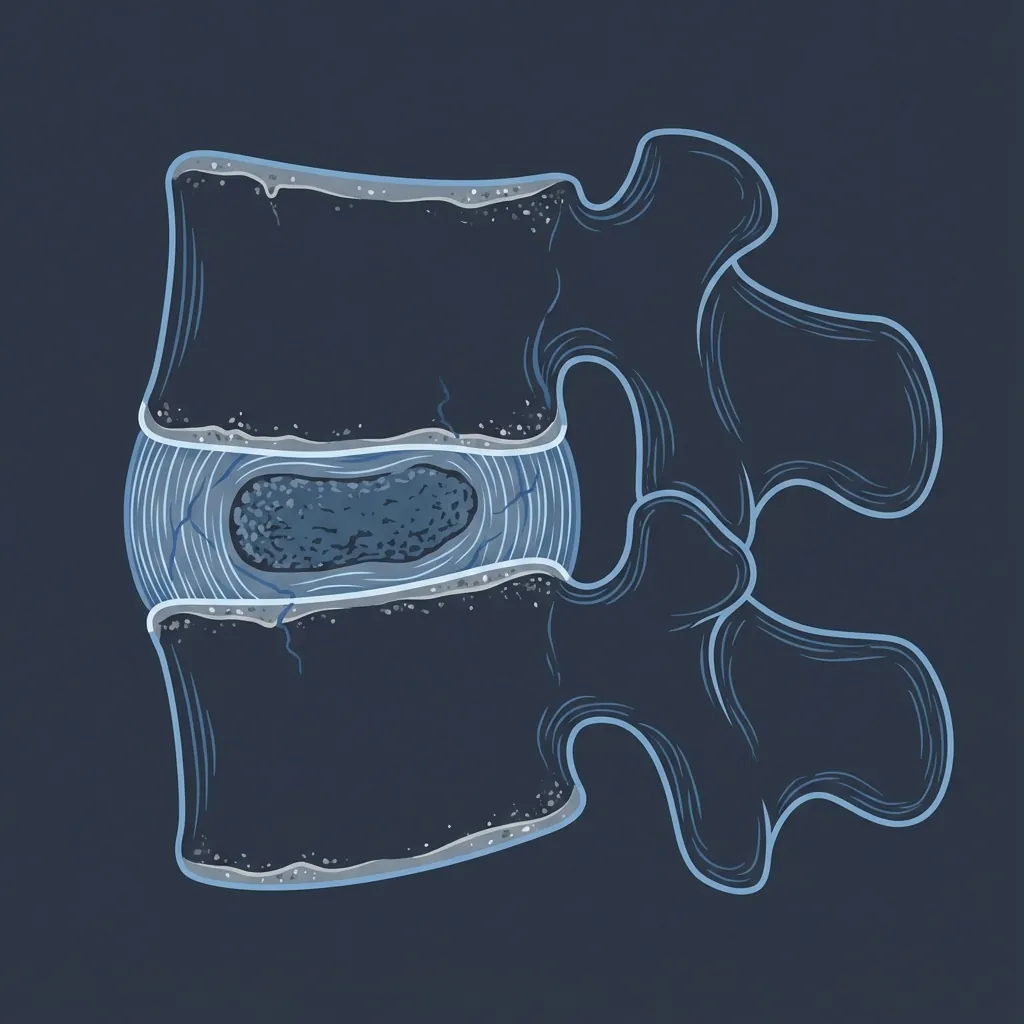
How Discs Function: The Foundation
The spine is connected by intervertebral discs—sophisticated biological structures positioned between each vertebra.
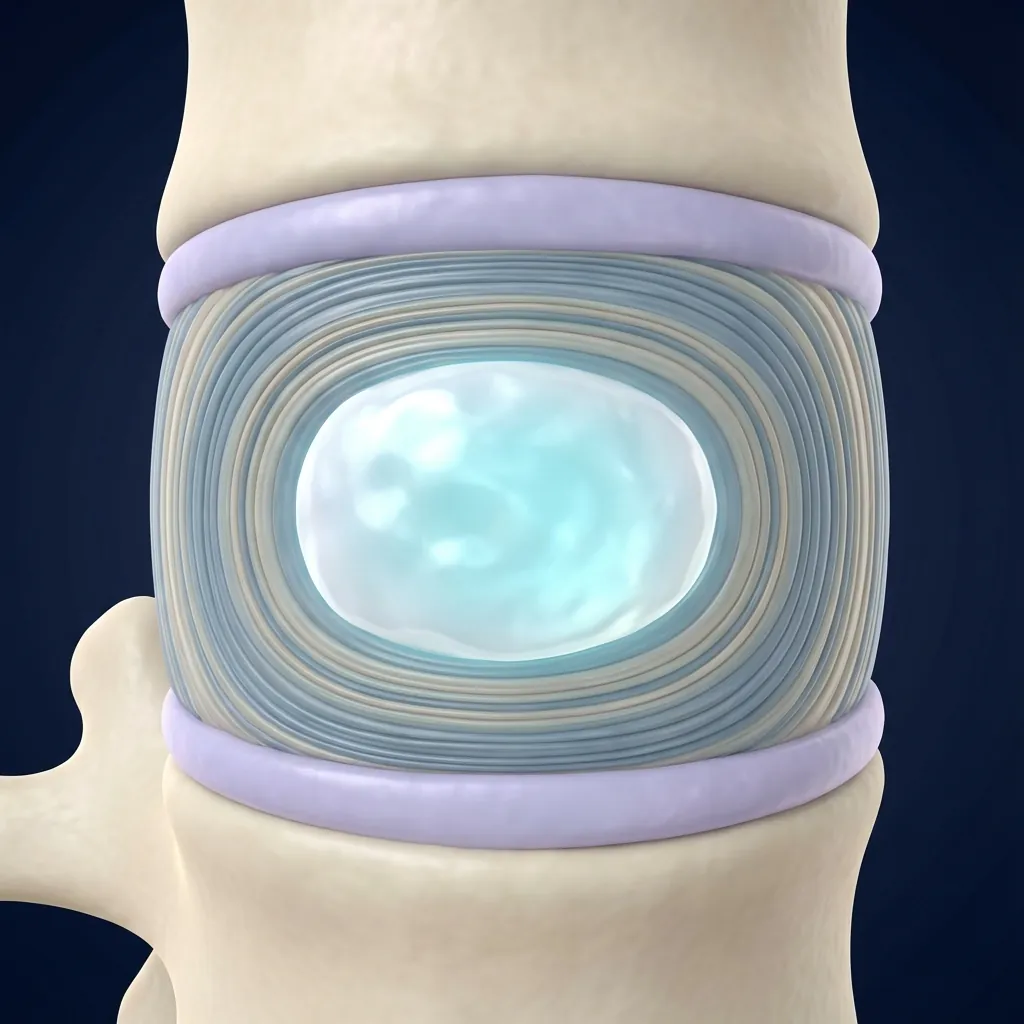
The Nucleus Pulposus
The gel-like centre, composed of approximately 80% water. It functions like a hydraulic shock absorber, cushioning every movement.
The Annulus Fibrosus
The tough, fibrous outer ring—similar to a tyre's sidewall. Contains concentric collagen fibre layers that provide structural stability and keep the nucleus contained.
Key Functions
Absorb Shock
with spinal movement
The gel-like nucleus pulposus compresses and redistributes forces during activities like walking, running, or lifting.
Allow Motion
flexion, extension, rotation
Discs enable the neck to move freely—looking up, down, and side to side—while maintaining stability.
Distribute Loads
evenly across the spine
Forces are spread across the entire disc surface, preventing concentrated stress on any single point.
Protect Nerves
maintaining proper spacing
By keeping vertebrae properly separated, discs protect the spinal cord and nerve roots travelling through the vertebral canal.
"This system has evolved over millions of years to be remarkably efficient. When functioning properly, individuals can move the neck freely, absorb impacts, and maintain comfortable function for decades."
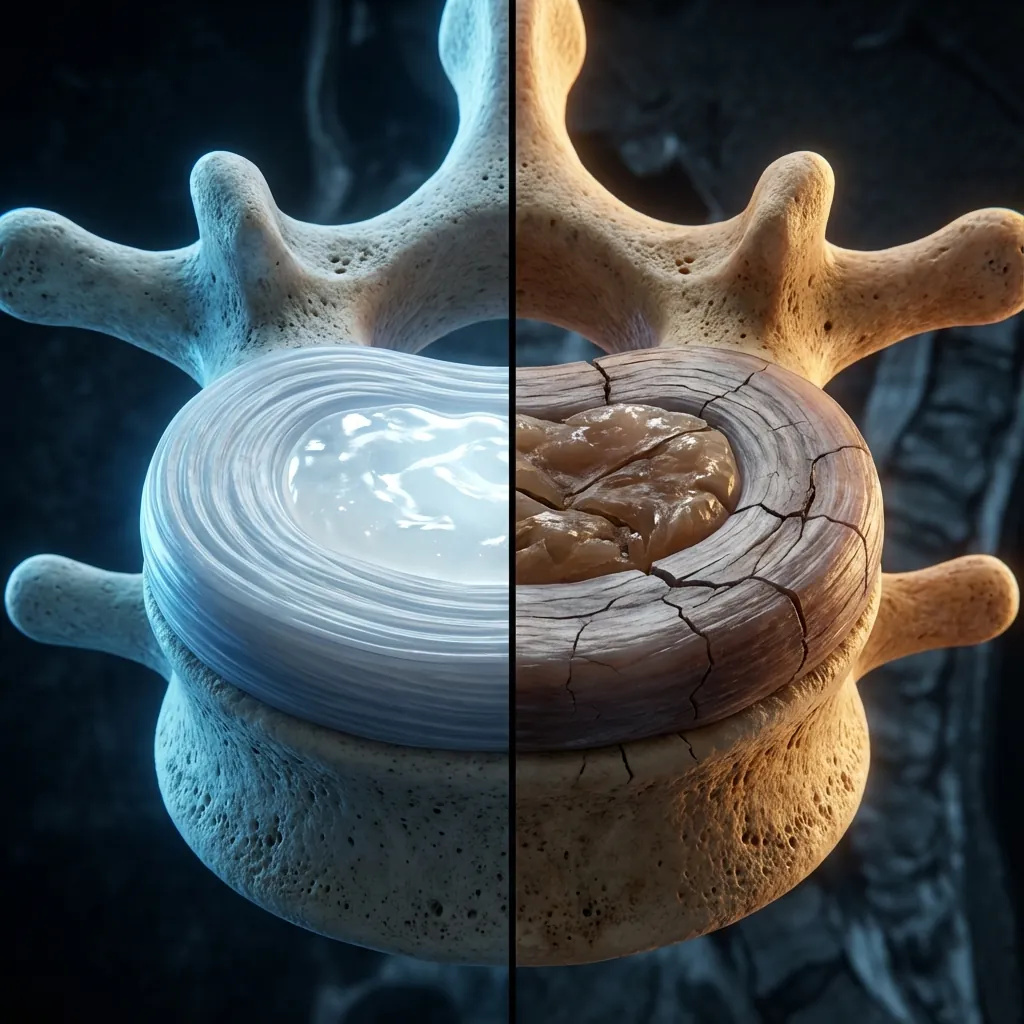
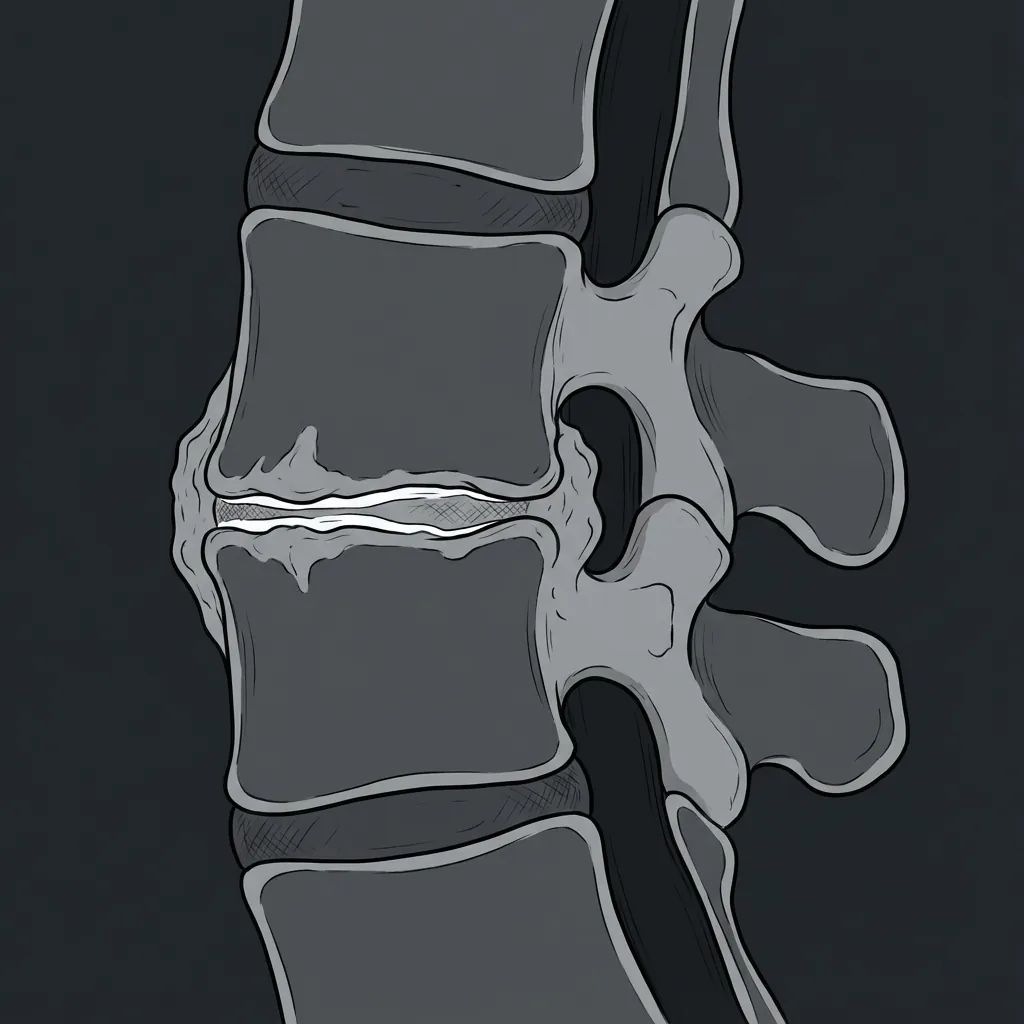
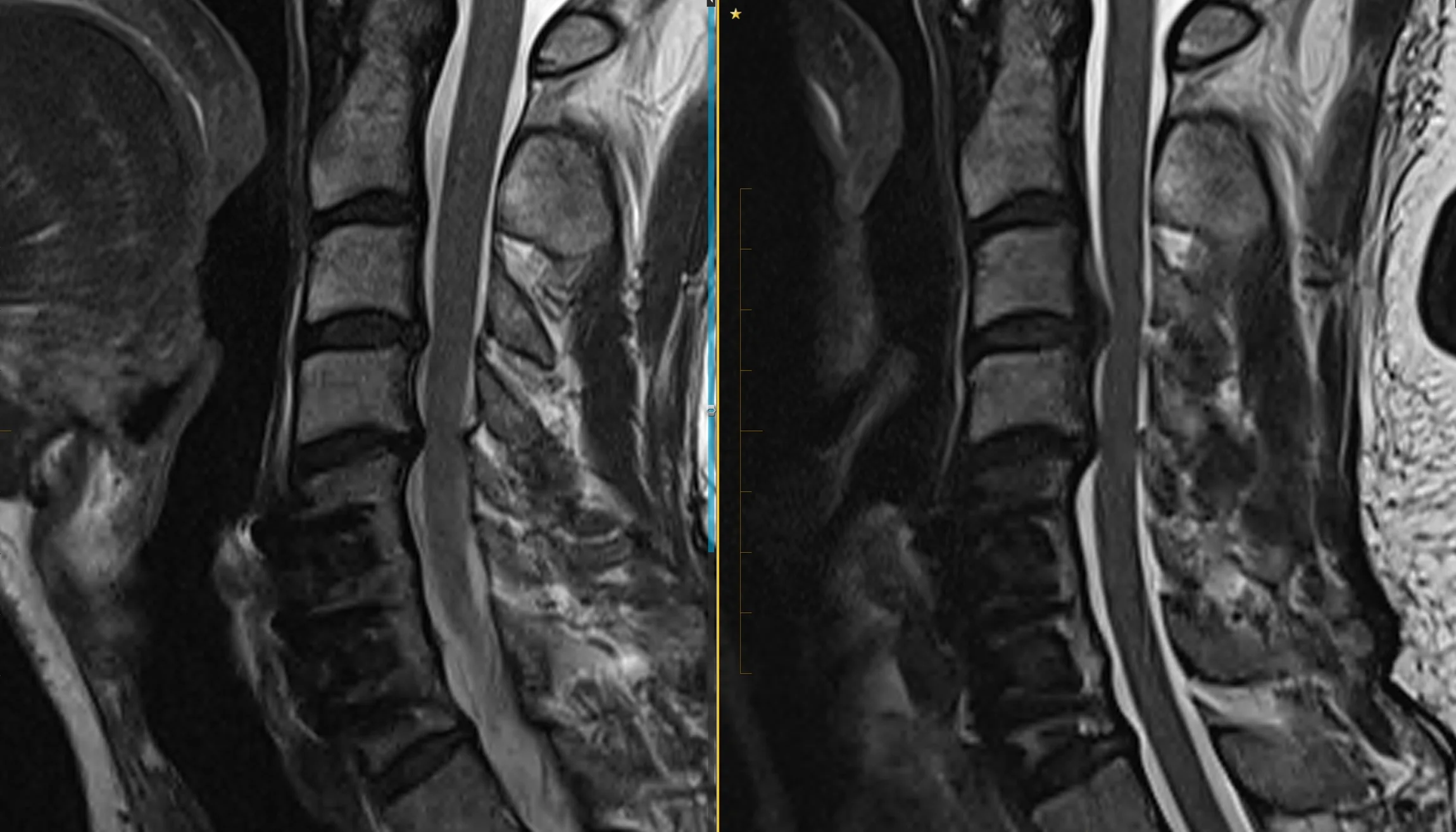
When Discs Fail
Disc degeneration becomes problematic when structural changes cause pain or compress nerve structures. The typical progression follows this pattern:
Dehydration
Water loss begins silently
The nucleus pulposus gradually loses water content—a process beginning in the 20s or 30s but typically causing no symptoms until later decades. As hydration decreases, the disc becomes less effective at shock absorption and loses height.
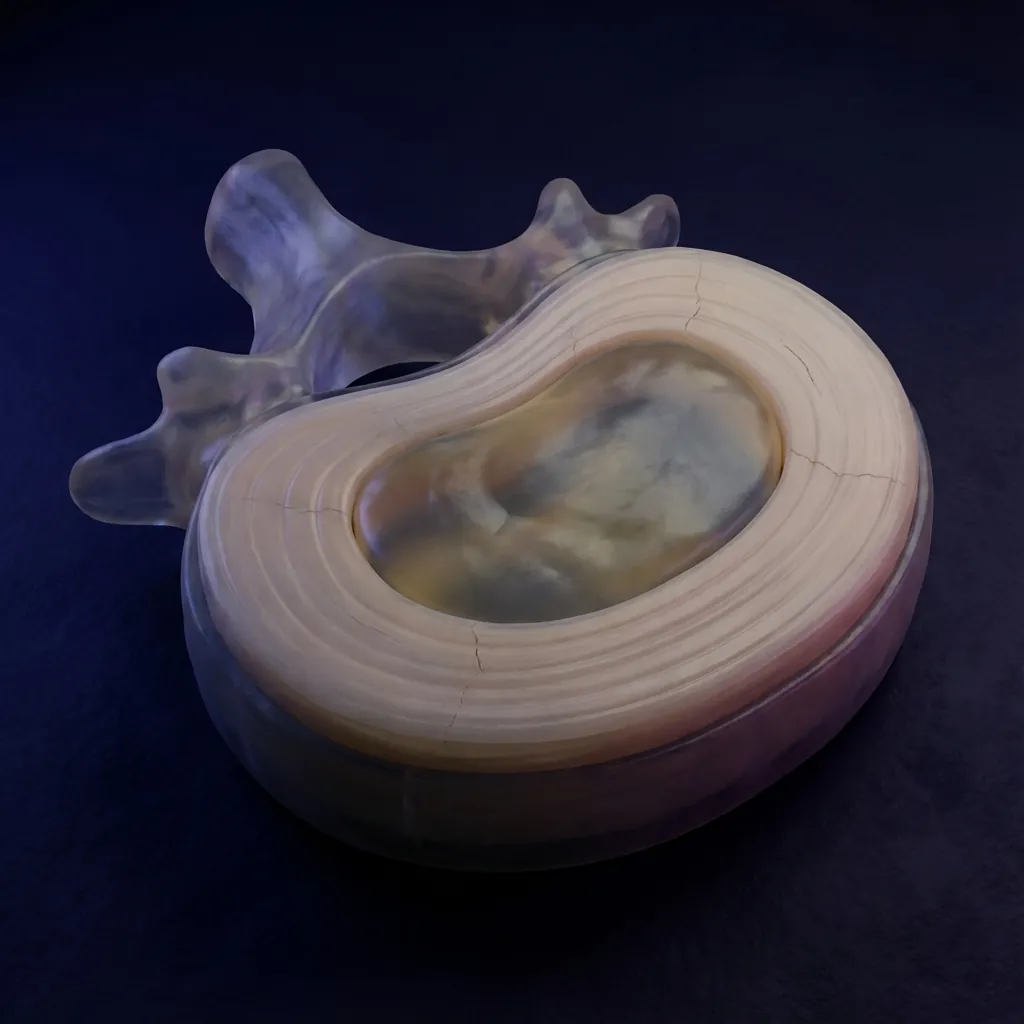

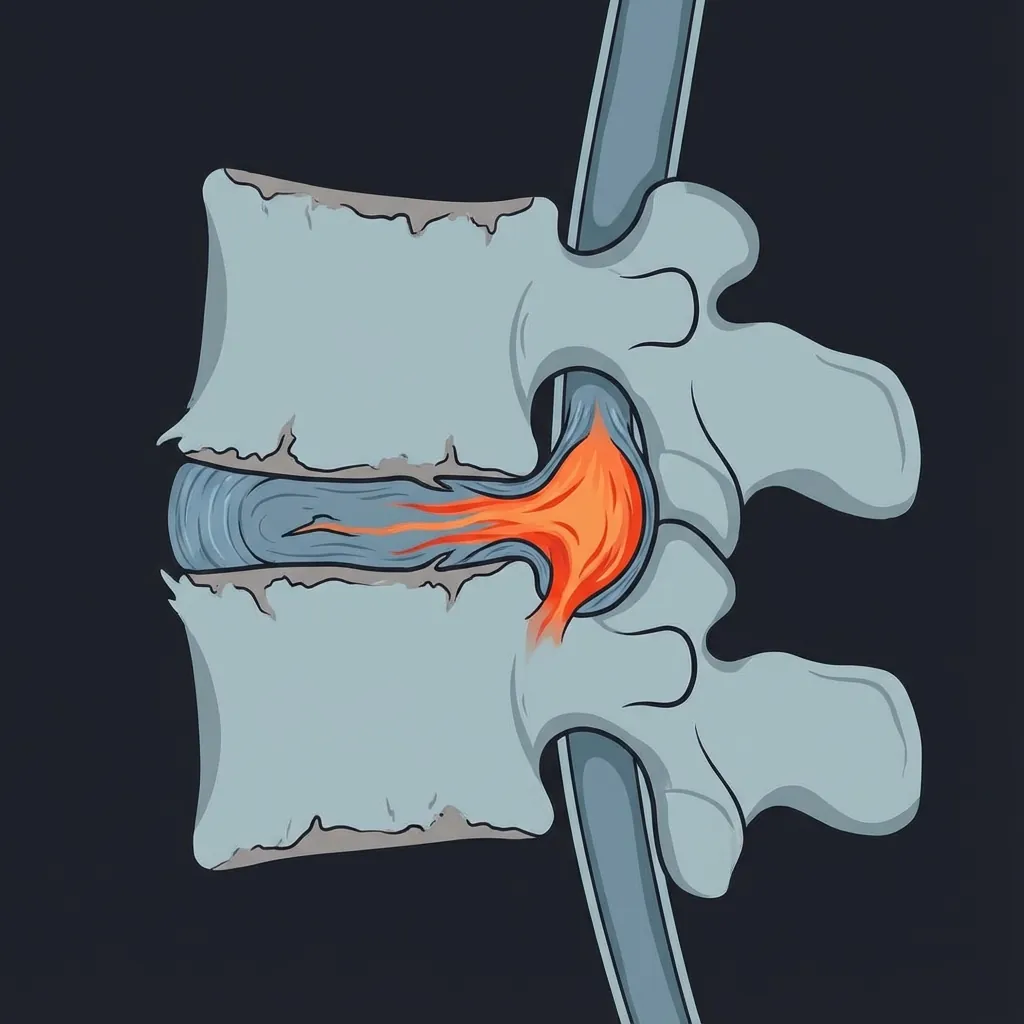
Structural Changes
Cracks and tears develop
As the disc loses height and hydration, the annular fibres can crack or tear. Nucleus material can herniate through these tears, pressing outward into the spinal canal or lateral recesses where nerve roots travel. Additionally, the body responds by forming osteophytes (bone spurs) at vertebral margins.
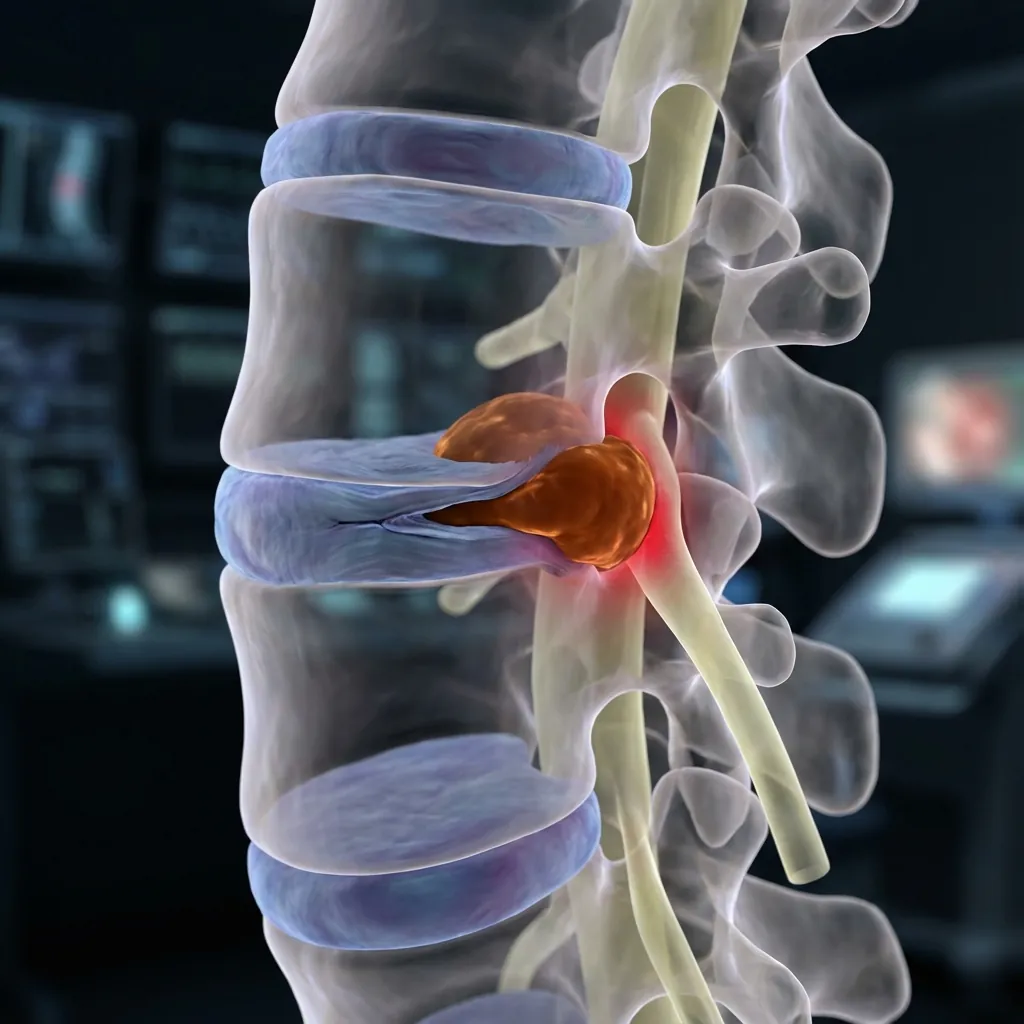
Neural Compression
Nerves become affected
Herniation and bone spurs press against the spinal cord (myelopathy—causing clumsiness, balance problems, weakness) or nerve roots (radiculopathy—causing pain, numbness, tingling down the arm).
Two Philosophies
When conservative treatment has failed and symptoms are significant enough to warrant surgery, patients typically face two main options representing fundamentally different approaches.
Spinal Fusion
Surgeons remove the damaged disc and permanently fuse the two vertebrae together, typically using bone graft material and metal plates and screws. The vertebrae essentially become one solid bone unit with no motion between them.
Advantages:
The Trade-off:
Fusion solves the immediate problem but creates a permanent consequence: the treated segment becomes completely rigid. The vertebrae above and below this fused segment must now do more work to compensate.
Adjacent Segment Disease
Over 10–20 years, this accelerated wear leads to degeneration at those adjacent levels in 25–30% of fusion patients, often requiring additional surgery.

Arthroplasty
Surgeons remove the damaged disc and replace it with an artificial disc implant—a sophisticated mechanical device designed to restore the disc's function. Rather than eliminating motion, the implant maintains the spine's natural motion while fixing the problem causing pain and nerve compression.
How It Works:
The artificial disc typically has metal endplate components (that interface with the vertebral bodies above and below) and a polyurethane or ultra-high molecular weight plastic articulating surface.
Advantages:
The Requirement:
Arthroplasty is appropriate for 1–2 consecutive levels of disease with adequate bone quality and relatively healthy facet joints. It's not suitable for all patients.
Head-to-Head Comparison
A direct comparison of outcomes based on long-term clinical studies.
See why arthroplasty is the modern standard for eligible patients.
| Parameter | Arthroplasty | Fusion |
|---|---|---|
| Motion at Treated Level | Preserved (85–90% normal) | Eliminated (rigid) |
| Adjacent Segment Stress | Normal distribution | Increased 15–25% |
| Adjacent Segment Disease Risk | 5–10% at 10 years | 25–30% at 10 years |
| Pain Relief | 80–90% improvement | 85–95% improvement |
| Reoperation Rate | 3–7% at 10 years | 15–25% at 10 years |
| Long-term Function | Maintained mobility | Increasing stiffness |
| Track Record | 20+ years | 50+ years |
| TGA/FDA Approval | 1–2 levels (approved devices) | All cervical disease |
The Bottom Line
Both approaches achieve excellent pain relief. The key difference lies in long-term spinal health: fusion trades motion for immediate stability, while arthroplasty preserves motion to protect adjacent segments and maintain function into your 60s, 70s, and beyond.
Why Discs Fail
Disc degeneration is a normal process. Just as cliffs erode from wind and rain, intervertebral discs weather with time.
It begins earlier than expected—often in the 20s—but typically stays silent until middle age.

"Biological structures follow the same laws of entropy as the earth itself."
The Elements of Decay
Multiple forces converge to accelerate the aging process.
Genetics
The internal blueprint. Family predisposition plays a major role.

Mechanical Wear
Repetitive movements and high-impact activities.

Injury History
Trauma accelerates local degeneration.

Lifestyle
Smoking and nutrition affect disc health.

Time
The unavoidable biological passage.
Individual Landscapes
Two people. Same age. Completely different experiences.
The Clinical Insight
Imaging ≠ Pain. A degenerative MRI does not automatically require treatment. We treat the patient, not the picture.

“Lives completely symptom-free despite 'scary' MRI findings.”

“Experiences significant daily pain despite 'normal' imaging.”
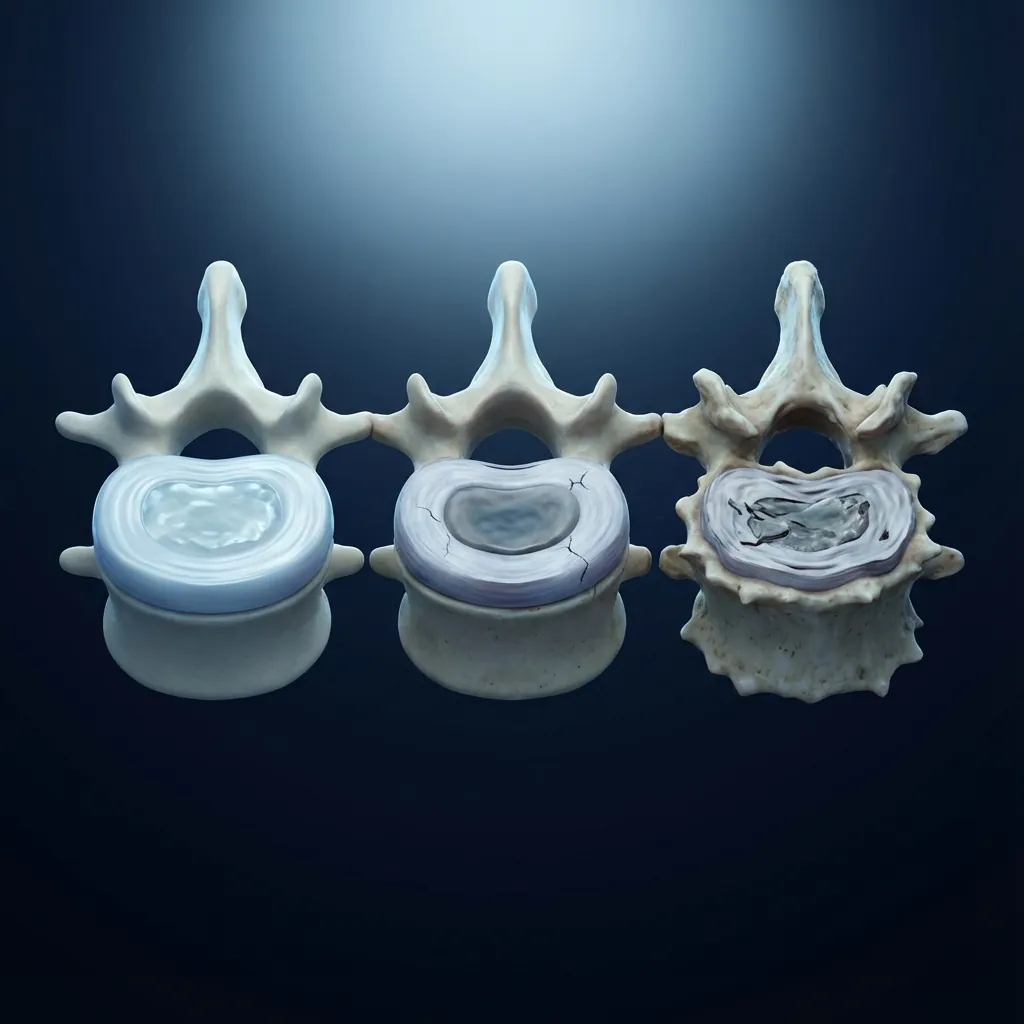
The Stages
A descent into deeper structural change. Select a stage to explore the erosion process.

The Baseline
Normal Disc
The Baseline
"A smooth, unweathered river stone."
Early Shift
"Fine hairline cracks appearing in the surface."
Structural Break
"A deep fissure splitting the rock face."
The Collapse
"The structure begins to crumble and settle."
New Stasis
"Petrified, fused, and immobile."
When Structure Affects Function
Erosion becomes a problem only when it encroaches on the nervous system.
Radiculopathy
Nerve Root Compression. Like a rock trapping a specific root.
- Pain radiating down arm
- Numbness in specific area
- Tingling sensations
- Focal weakness
Myelopathy
Spinal Cord Compression. A blockage of the main channel.
- Balance difficulties
- Global weakness
- Clumsiness
- Neurological decline
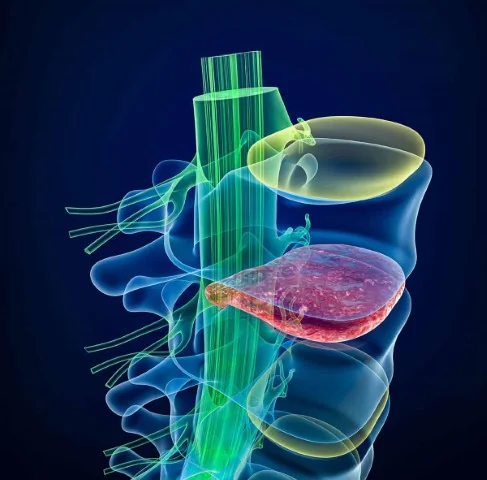
Anatomical Reality
Whether it's the nerve root (Radiculopathy) or the cord itself (Myelopathy) dictates the urgency and type of surgical intervention required.
Why Motion Matters Beyond Pain Relief
While both fusion and arthroplasty effectively relieve pain, they differ dramatically in what happens to the spine over 10, 20, and 30 years.
This isn't about short-term outcomes—it's about protecting your spine for decades to come.
"The real advantage of motion preservation isn't just better 2-year outcomes— it's dramatically better 20-year and 30-year outcomes."
50–70%
Risk Reduction
Adjacent Segment Disease
When fusion eliminates motion at one level, the work that segment used to do gets redistributed—accelerating wear at neighboring levels.
Higher Long-term Risk
25–30%
10-Year ASD
30–40%
15-Year ASD
15–25%
Reoperation
When fusion eliminates motion at one level, adjacent segments compensate—experiencing 15–25% more motion. This accelerated wear leads to degeneration cascade.
Protected Adjacent Levels
5–10%
10-Year ASD
10–15%
15-Year ASD
3–7%
Reoperation
Motion preservation maintains normal load distribution. Adjacent segments function as designed, dramatically reducing long-term disease risk.
The Cascade Effect
What happens mechanically over time
Accelerated disc degeneration
Herniation and stenosis
Osteophyte formation
Neurological symptoms at new levels
Why This Matters for Long-Term Outcomes
A 50-year-old patient undergoing fusion might develop symptomatic problems at adjacent levels by age 60–65, creating difficult treatment choices. The same patient with arthroplasty is statistically more likely to have a single successful surgery with protected adjacent segments, rather than a series of surgeries addressing progressive degeneration.
Equal distribution across all segments
Coordinated movement preserved
Why Motion Preservation Protects
Fusion Issue
Adjacent segments bear above-normal loads throughout daily activities.
Arthroplasty Benefit
All segments share proportional load—no single segment overloaded.
Visual Metaphor: Like a relay team where all runners share the workload equally.
Long-Term Motion Preservation
Decades of follow-up data answer the critical question: Do artificial discs maintain function long-term? The answer is definitively yes.
PRESTIGE LP
FDA Trial Data • 7+ Years Follow-up
85–90%
Motion Preserved
Confirmed
No Progressive Stiffening
93%
Patient Satisfaction
2.9% vs 4.9% fusion
Adjacent Segment Disease
ProDisc-C
Randomized Trial • 10+ Years Follow-up
Documented
Motion Preservation
Superior to fusion
Patient Outcomes
Low
Complication Rate
Maintained
Long-term Stability
Charité Lumbar
International Data • 10+ Years Follow-up
85%
Normal Motion
None
Device Failures
Confirmed
Implant Durability
Predictable
Outcomes
Is Arthroplasty Right for You?
Spinal arthroplasty is an excellent option for many people, but it's not right for everyone. Rather than assuming surgery is necessary, this section helps you understand the clinical criteria that determine suitability.
Likely Suitable
— Strong CandidatePatients who meet key clinical criteria and can expect excellent outcomes from arthroplasty.
Medical suitability isn't binary—it's not simply 'yes' or 'no.' Rather, it exists on a spectrum. Most patients fall somewhere in between.
Understanding Your Position
Explore each assessment area to understand how candidacy is determined. Click any item for detailed information.
You're Probably Suitable If...
Click each criterion to learn more
5 minute self-assessment
Summary Profiles
Where do you fall on the spectrum? These profiles summarize the typical patient categories.
Likely Suitable
Strong candidates with excellent outcomes expected
- 1–2 level disc disease
- Adequate bone quality
- Relatively healthy facet joints
- Discogenic pain pattern
- Adequate medical health
Worth Discussing
May benefit with additional evaluation or optimization
- Mild osteoporosis (can be optimized)
- Grade 2–3 facet arthritis (SPECT/CT can clarify)
- Multiple levels affected
- Significant medical comorbidities
May Not Be Suitable
Contraindications present or significant risks
- Severe osteoporosis (T-score < -3.5)
- Grade 4 facet arthritis with metabolic activity
- 3+ levels of significant disease
- Severe medical comorbidities
Every Patient is Unique
These criteria provide a framework, but the final determination requires a detailed clinical assessment. Imaging findings, physical examination, and patient goals all factor into the decision.
Many patients in the "worth discussing" category become excellent candidates after optimization—whether that means improving bone density, managing comorbidities, or clarifying the pain source with additional testing.
“We treat the patient, not the imaging. Your story matters as much as your MRI.

Arthroplasty makes things
substantially better, not perfect.
Surgery doesn't reverse decades of degeneration—it addresses the current problem causing your symptoms whilst protecting your spine's future health.
Most patients describe it as life-changing in positive ways, but realistically, you're trading one set of circumstances (your degenerative disc problem) for a different set (a surgically treated spine with an implant).
The evidence clearly shows this trade-off is worthwhile for most suitable candidates, but it's important to go in with accurate expectations.
"We don't promise perfection—we promise honest assessment and the best possible outcome for your individual situation."
Path to Restoration
Recovery isn't a single event—it's a structured journey. Understand the timeline from diagnosis to full function.
Assessment
The journey begins with acknowledging symptoms and seeking initial evaluation.
Stage Goal
Realistic Expectations
Outcomes based on clinical data
Pain Relief
- Significant improvement80–90%
- Modest/Persistent10–20%
- Most improvement by 3 months.
Return to Function
- Light Work4–6 Weeks
- Full Work8–10 Weeks
- Sports/High Impact3–6 Months
Neurological
- Radicular Pain: Weeks
- Motor Weakness: 3–6 Months
- Myelopathy: 6–12 Months
What Won't Recover
Permanent nerve damage (long-standing weakness/numbness) may not fully recover.
Chronic pain with psychological components may require ongoing management.
Three Decisions That Shape Your Path Forward
Every patient's situation is unique. Here are three decisions to think through as you consider your options—real, important decision points in your treatment journey.
Do I Actually Need Surgery?
The first and most fundamental question
Conservative Management Should Be Tried First If:
You're in the early stages of your problem (recent onset, less than 3 months)
Your symptoms are mild to moderate
You haven't experienced progressive neurological changes
Your imaging shows changes but is stable and not severe
You've shown good initial response to treatment
Reality check: Many people have abnormal-looking discs on imaging but don't need surgery. They manage their symptoms with conservative care and do well long-term.
In these situations, your body may be capable of healing naturally with proper support. Rushing into surgery when conservative care might work is unnecessary.
Motion Preservation or Fusion?
Once you've decided surgery makes sense
Both disc replacement and fusion successfully address nerve compression and relieve pain. They differ in how they reconstruct your spine and what happens long-term.
Disc Replacement
Maintains your spine's natural movement at the treated level whilst protecting adjacent segments from excess stress.
Who It's Best For
Evidence-Based Outcomes
Commitment required: You need to commit to reasonable activity guidelines post-operatively. Your implant is very durable, but like any joint, it performs best when used appropriately.
Spinal Fusion
Permanently fuses two or more vertebrae together, eliminating motion at that level but creating permanent stability.
Who It's Better For
Historical Data
The Honest Conversation
Your surgeon will assess your specific anatomy, imaging, bone quality, and medical situation. The "best" approach is the one that works for your spine and your situation, not what works in general. If you have reasonable bone quality, one or two levels of disease, and want to preserve motion, arthroplasty is typically ideal. If you have multiple levels involved or other complicating factors, fusion may be recommended.
Ready to Move Forward?
Three pathways based on your readiness
Different people are ready at different stages. Here are three ways to proceed, depending on where you are.
Still Exploring Your Options
You're not sure yet, want to understand more before deciding, or want to be thorough in your research.
What You'll Do:
Browse our comprehensive patient learning library
Read detailed guides about your condition and treatment options
Understand how disc degeneration progresses
Learn what different symptoms mean
Take your time making an informed decision
20–40 minutes depending on depth
None—just learning at your own pace
The Diagnostic
Observatory
Standard MRI and CT reveal structure—but optimal candidacy assessment requires seeing function, density, vessels, and biochemistry. Five advanced technologies ensure the right patients receive the right treatment.
Nociscan MRI
Non-Invasive Disc Analysis
Revolutionary technology that identifies painful discs through biochemical analysis—without needles, contrast, or patient discomfort.
Comprehensive Candidacy Assessment
These advanced diagnostics ensure we see the complete picture before recommending surgery. Not every patient needs every test—your assessment is tailored to your specific clinical presentation.
Flexion/Extension X-Rays
Dynamic imaging represents a cornerstone of spinal biomechanical assessment, providing functional information unavailable from static imaging studies. These studies evaluate segmental motion patterns, detect instability, and inform treatment decisions in degenerative spine disease.
Technical Execution
Patient Positioning
- Patient positioned standing (allows gravity's natural loading)
- Lateral cervical or lumbar radiographs taken
- Initial image in neutral (relaxed) standing position
- Second radiograph at maximum forward flexion
- Third radiograph at maximum backward extension
Image Quality Considerations
- Proper exposure essential (underpenetrated films may obscure subtle motion)
- Consistent magnification maintained throughout series
- Patient cooperation critical (genuine maximal flexion/extension required)

Normal Segmental Motion Ranges
Flexion/extension images enable measurement of intervertebral motion at each spinal level
| Spinal Region | Normal Motion Range |
|---|---|
| Cervical (per level) | 8–12 degrees |
| Lumbar L1–L4 (per level) | 10–15 degrees |
| Lumbar L5–S1 (per level) | 5–10 degrees |
Motion Patterns Identified
Understanding motion abnormalities is critical for surgical planning
Hypermobility
Definition: Segmental motion exceeds normal range
Causes
- Ligamentous laxity
- Advanced disc degeneration
- Post-surgical changes
Clinical Significance
Suggests instability or ligamentous laxity
Disc Replacement Perspective
May indicate fusion more appropriate than disc replacement in certain presentations
Example
L4–L5 motion of 25° (normal ~12°) suggests hypermobility
Hypomobility
Definition: Segmental motion less than expected
Causes
- Osteophytes limiting motion
- Degenerative stiffening
- Post-fusion rigid segment
Clinical Significance
Suggests mechanical restriction
Disc Replacement Perspective
If motion loss attributable to osteophytes only (not facet pathology), disc replacement can restore motion
Example
L3–L4 showing only 3° motion due to large osteophytes
Rigid Segment
Definition: No visible motion between vertebrae on flexion/extension
Causes
- Severe degeneration
- Previous fusion
- Advanced osteophytosis
Clinical Significance
Complete loss of segmental motion
Disc Replacement Perspective
If rigid from degenerative stiffness (not fusion hardware), motion restoration through disc replacement offers potential benefit
Example
Complete absence of motion at affected segment
What Flexion/Extension X-Rays Reveal
Comprehensive biomechanical analysis beyond static imaging
Subluxation & Slip Assessment
Detects forward slipping of vertebrae (spondylolisthesis or vertebral translation)
Kyphotic/Lordotic Alignment
Shows changes in regional spinal curvature with movement
Neutral Zone Assessment
Advanced analysis of the motion region without segmental resistance
Osteophyte Motion Restriction
Reveals how bone spurs affect motion patterns
Advantages of Flexion/Extension X-Rays
Functional Assessment: Only imaging showing dynamic motion patterns
Instability Detection: Gold standard for identifying mechanical instability
Radiation Efficiency: Minimal radiation (2–3 images vs. multiple CT slices)
Cost-Effective: Inexpensive compared to advanced imaging
Easy Interpretation: Clinicians readily understand motion patterns
Why Trust Arthroplasty?
Spinal arthroplasty isn't experimental. It's evidence-based surgery with over 20 years of clinical experience and rigorous research. Thousands of patients have been followed through long-term trials. The data consistently demonstrates superior outcomes compared to traditional fusion.
Foundation of Confidence
This data comes from peer-reviewed research published by independent researchers following thousands of patients through FDA rigorous trials and international registries—not manufacturer marketing.
Why Trust Arthroplasty?
Trust isn't given—it's earned through transparency, evidence, and demonstrated outcomes. The case for motion-preserving disc replacement is built on rigorous clinical trials, long-term follow-up data, and decades of real-world results.
The Evidence, The Innovation, The Track Record
Multiple large clinical trials comparing arthroplasty to fusion demonstrate consistent findings across pain relief, function, and long-term spinal health.
Approved & Validated
Motion-preserving disc implants have undergone rigorous regulatory evaluation in both the United States and Australia.
FDA Approved
Following rigorous FDA Investigational Device Exemption (IDE) trials and comprehensive evaluation, motion-preserving discs have been approved in the United States.
- Over 20 years of regulatory oversight
- Comprehensive clinical safety monitoring
- Rigorous IDE trial requirements met
TGA Approved
Motion-preserving discs are approved and available in Australia after comprehensive evaluation by the Therapeutic Goods Administration.
- Recognised as safe and effective
- Within Australian regulatory framework
- Ongoing post-market surveillance
Key Findings
Peer-reviewed research published in respected medical journals including Spine, European Spine Journal, and Neurosurgery.
Motion Maintained at 10+ Years
Long-term imaging and biomechanical studies show artificial discs maintain 85–90% of normal spinal motion at the treated level over 10+ year follow-up. Implants continue functioning properly without becoming stiff.
Lower Adjacent Segment Disease
Compared to fusion, patients with disc replacement experience 50–67% reduction in developing problems at discs adjacent to the treated level over 10 years. This is a substantial difference in long-term spinal health.
Reoperation Rate at 10 Years
Motion-preserving surgery requires reoperation at rates of 3–7% at ten years. By contrast, fusion patients have reoperation rates of 15–25%, predominantly due to adjacent segment disease.
Patient Satisfaction in RCTs
When patients who received arthroplasty are compared directly to fusion patients in rigorous randomised studies, arthroplasty patients report higher satisfaction scores, better outcomes, and superior quality of life.
Long-Term Data
The longest and most rigorous studies show that artificial discs maintain function long-term. Here's what decades of follow-up reveal.
Why Surgeons Recommend It
- Excellent pain relief (80–90%)
- Faster functional recovery
- Protected adjacent segments (50–70% lower risk)
- Maintained spinal mobility
- Preserved spinal health for decades
- Lower lifetime surgery burden
- Pain relief and preserved mobility
- Maintained spinal functional capacity
- Avoid the cascade of degenerative changes
Who Performs Your Surgery
Dr Ales Aliashkevich specialises in spinal arthroplasty with extensive experience in motion-preserving procedures.
Cervical Disc Replacement
Lumbar Disc Replacement
Volume & Complexity
Hundreds of motion-preserving procedures completed, with particular expertise in complex cases and multilevel surgeries.
Multidisciplinary Approach
For lumbar procedures requiring anterior access through the abdomen, Dr Aliashkevich collaborates with experienced vascular surgeons who specialise in approaching the lumbar spine safely whilst managing major blood vessels. This teamwork ensures safety and excellent outcomes.
Not everyone needs surgery. Not everyone who needs surgery should have arthroplasty. The goal is finding the right treatment for your specific situation—whether that's conservative management, motion preservation, or fusion. I'm committed to honest patient selection and individualised treatment planning.
Experience & Credentials
- Exclusive focus on spinal arthroplasty
- Ongoing training and education in latest techniques and implant technology
- Active involvement in medical societies focused on motion preservation
- Commitment to following best international standards and practices
The Decision Process
A considered, step-by-step approach ensures the right treatment for your specific situation.
What the Evidence Shows
Arthroplasty works:
- 80–90% of patients experience significant pain improvement
- Motion is preserved long-term (85–90% at 10+ years)
- Adjacent segments are protected (50–70% lower risk vs. fusion)
- Patient satisfaction is high (93%)
“For the right patient, arthroplasty offers a superior biological solution by maintaining the spine's natural kinematics whereas fusion creates a permanent biomechanical alteration.”
Ready to Discuss Your Options?
Every patient case is unique. The best way to understand if you are a candidate for arthroplasty is through a comprehensive specialist evaluation.
Informed Decisions, Better Outcomes
The Spine Deserves Better—And So Do Patients
Chronic spine pain doesn't have to mean sacrificing mobility.
Fusion works, but it's not the only answer. Motion-preserving disc replacement offers pain relief and preserved function.
But it's not for everyone:
- Some patients need fusion (severe degeneration, multiple levels, severe facet arthritis)
- Some patients should continue conservative management (good response to treatment)
- Some patients have contraindications (severe osteoporosis, poor medical health)
The Real Advantage
The real advantage of motion preservation isn't just better 2-year outcomes—it's dramatically better 20-year and 30-year outcomes.
A 50-year-old with arthroplasty is more likely to have a single successful surgery at age 50 with protected adjacent segments for the next 30+ years.
A 50-year-old with fusion is more likely to face a series of surgeries over the next 30 years as adjacent-segment disease develops.
That's the fundamental difference.