
Preoperative Assessment Cervical Disc Replacement
The systematic clinical and diagnostic process that determines who is a suitable candidate for cervical disc replacement, what needs to be done surgically, and how to minimise risks and optimise outcomes.
Assessment Timeline
Consultation to Surgery
4-8 Weeks
Comprehensive pathway from initial consultation through imaging, testing, optimisation and final pre-operative visit.
Success Rate
Excellent Outcomes
85-95%
Patients with thorough preoperative assessment experience fewer complications, faster recovery and superior long-term results.
Team Approach
Collaborative Care
Multidisciplinary
Spine surgeon, anaesthesiologist, neurologist, radiologist and allied health professionals working together for optimal outcomes.
The Preoperative Assessment JourneyWhy Assessment Matters
Preoperative assessment is not bureaucratic delay—it's surgical preparation. Every element of your assessment directly influences whether disc replacement is right for you, which approach works best, what risks apply, and how well you'll recover.
Rushed Assessment Leads To
- Wrong surgical decisions
- Increased complications
- Suboptimal outcomes
- Preventable revisions
Thorough Assessment Leads To
- Confidence in decision-making
- Optimised surgical planning
- Reduced complications
- Excellent long-term function
Assessment Timeline
4–8 weeks typical
Your Assessment Ensures
Clinical Evaluation FrameworkUnderstanding Your Symptoms
The surgeon begins by understanding what is bothering you and why—not just accepting your self-reported diagnosis. A thorough cervical spine examination includes inspection, palpation, range of motion, neurological testing and specialised manoeuvres.
Chief Complaint & Symptom Characterisation
Why This Matters
- • Localises problem: Specific dermatomal pattern suggests specific nerve root compression
- • Suggests urgency: Myelopathy symptoms (hand clumsiness, gait disturbance) are urgent
- • Assesses chronicity: Longstanding severe symptoms sometimes have worse outcomes
- • Sets expectations: Realistic functional goals improve satisfaction
Physical Examination Protocol

Motor Testing (Graded 0–5)
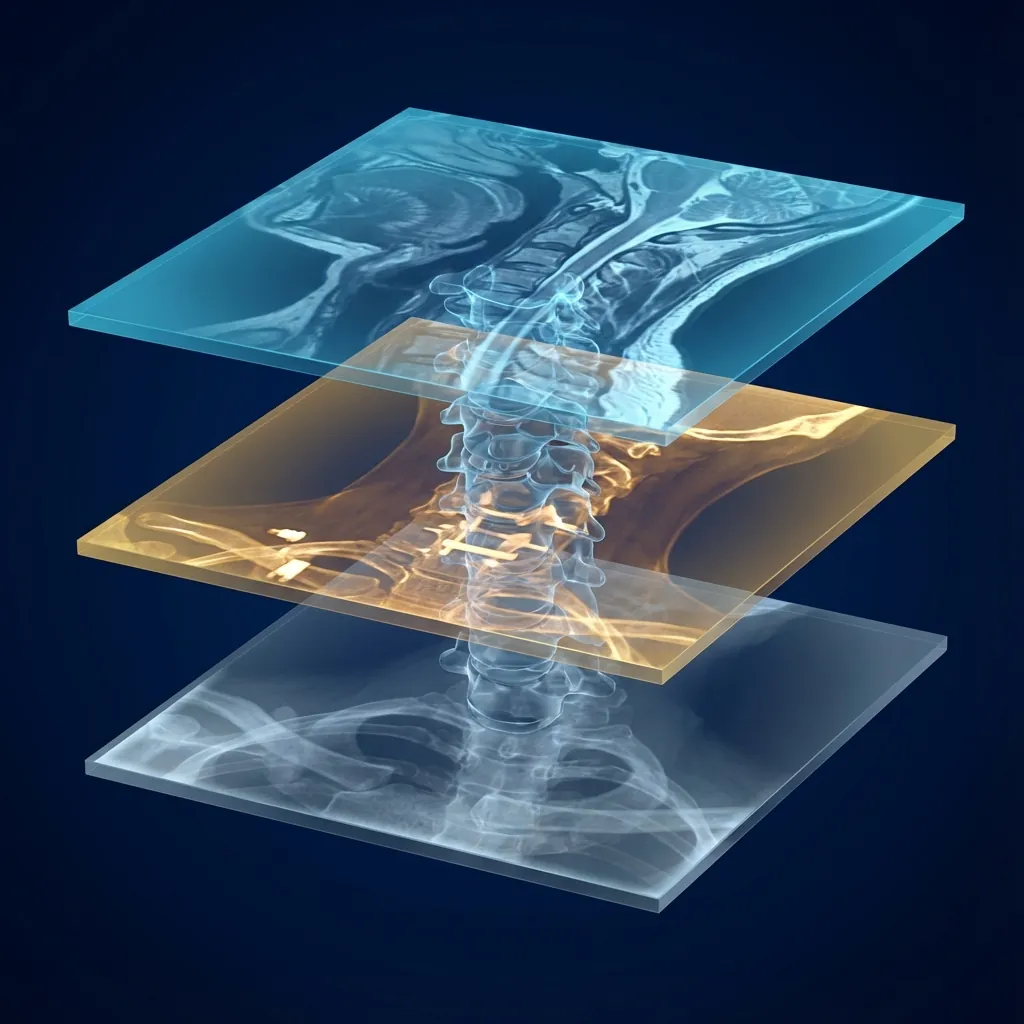
Diagnostic Imaging HierarchyLayered Diagnostic Intelligence
Each imaging modality reveals different aspects of your cervical spine pathology. Combined, they create a complete picture for surgical planning. Clinical correlation is essential—imaging must match symptoms.
MRI
The Soft Tissue Blueprint
What It Reveals
- Disc structure: Nucleus signal intensity (dark = desiccated, bright = hydrated)
- Disc height: Quantifiable disc space height
- Herniation pattern: Protrusion vs. extrusion; central, paracentral, or lateral location
- Spinal cord: Signal changes (T2 hyperintensity = cord edema or gliosis from compression)
- Nerve root: Compression, inflammation, signal changes
- Ligament status: PLL thickening, calcification; ligamentum flavum thickening
Limitations
- Cannot precisely show bone anatomy (cortical detail)
- Cannot clearly identify calcifications
- Overestimates stenosis in some cases
- Does not show dynamic compression (patient must be supine)
Asymptomatic disc herniations are common (30–50% of people without neck pain have MRI findings), so imaging must match symptoms.
DEXA T-Score Candidacy Guide
| T-Score | Classification | Arthroplasty Candidacy |
|---|---|---|
| > -1.0 | Normal bone | Excellent |
| -1.0 to -2.5 | Osteopenia | Good |
| -2.5 to -3.5 | Moderate osteoporosis | Questionable |
| -3.5 to -4.0 | Severe osteoporosis | Marginal |
| < -4.0 | Very severe osteoporosis | Contraindicated |
If osteoporosis is discovered, bone-strengthening medications can be started 3–6 months before surgery.
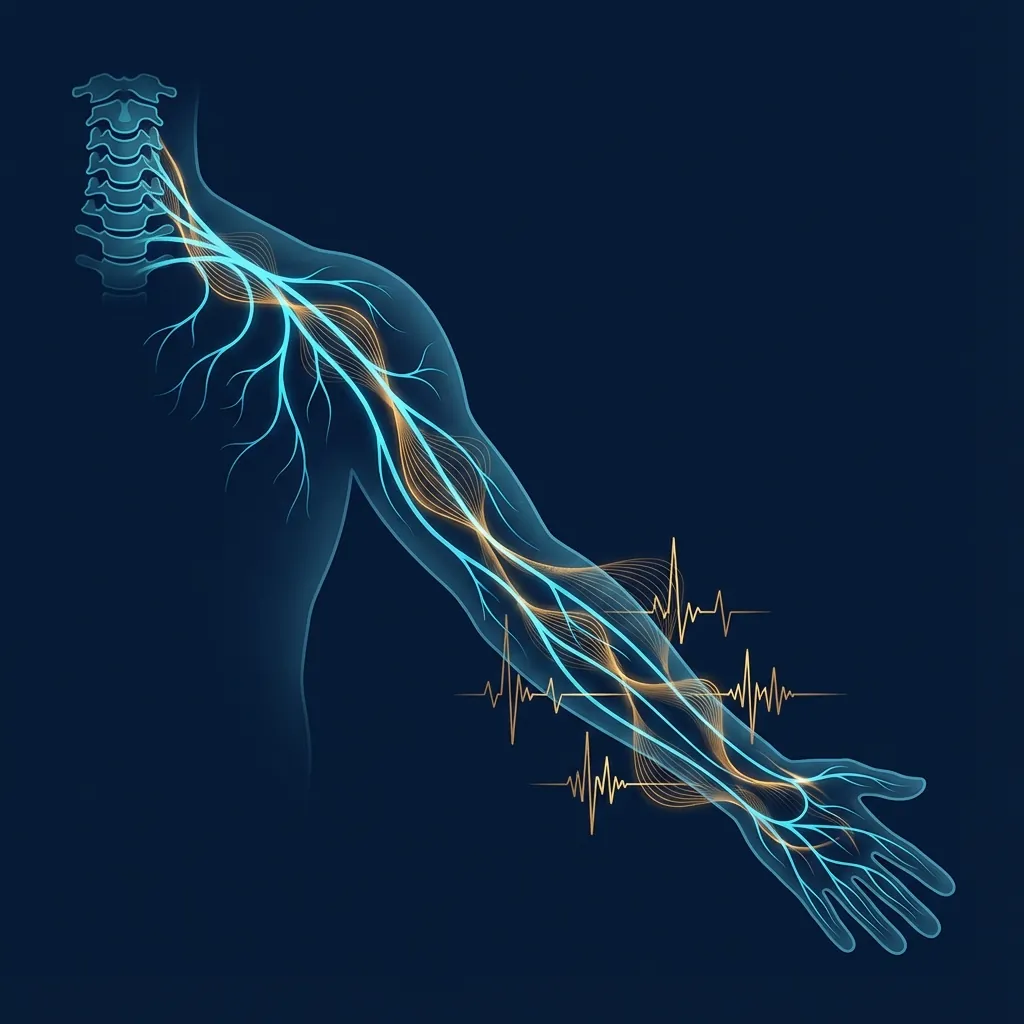
EMG and Nerve Conduction StudiesFunctional Confirmation of Imaging
While MRI shows structure, neurophysiological testing shows function. These tests determine whether nerves are actually being compressed and damaged—providing functional confirmation of imaging findings.
Nerve Conduction Studies
Measures how quickly and effectively electrical impulses travel along nerves.
How It Works
- 1Small stimulating electrodes placed on skin over a nerve
- 2Electrical stimulation applied (patient feels mild tingling)
- 3Recording electrodes at another location detect the response
- 4Latency and amplitude are measured and compared to normal values
Normal NCS in Cervical Radiculopathy
- This is expected and normal for most radiculopathy patients
- Compression occurs proximal to the dorsal root ganglion
- Normal NCS does NOT rule out cervical radiculopathy
Abnormal NCS Findings
- Slowed conduction velocity suggests demyelination
- Reduced amplitude suggests axonal injury
- F-wave abnormalities can detect root-level slowing
Sensitivity
Specificity
Cervical Radiculopathy Criteria
All of the following criteria must be met:
- 1Paraspinal muscle abnormalities: Fibrillations or positive sharp waves on needle EMG
- 2Peripheral nerve motor abnormalities: EMG abnormalities in 2 muscles innervated by same nerve root
- 3Different peripheral nerve distribution: Both muscles must be in different peripheral nerves
- 4Sensory NCS typically normal (expected finding)
- 5Motor NCS usually normal or mildly abnormal
Cervical Myelopathy Criteria
One or more of the following:
- 1SEP abnormalities: Delayed N13, abnormal P14, reduced amplitude (most specific)
- 2MEP abnormalities: Prolonged CMCT, reduced amplitude, asymmetry
- 3Combined SEP and MEP abnormalities (most specific for myelopathy)
- 4Correlation with clinical and imaging findings
Clinical Utility Note
EMG/NCS is most valuable when clinical diagnosis is unclear, multiple levels of compression exist, or peripheral nerve involvement may confound diagnosis. Test results also provide prognostic information—acute denervation patterns generally indicate good recovery potential, while chronic patterns suggest slower or incomplete recovery.
Patient Selection CriteriaWho Benefits from Disc Replacement?
Careful patient selection is crucial for optimal outcomes. Understanding who makes an ideal candidate, who requires careful consideration, and who should not undergo arthroplasty ensures the right surgical decision.

Ideal Candidates for Cervical Disc Replacement
Excellent candidates typically have these characteristics:
Clinical Decision Support
These criteria guide shared decision-making between you and your surgeon. Relative contraindications don't automatically exclude arthroplasty—they require careful evaluation, possibly additional testing (like SPECT/CT for facet arthropathy), and realistic discussion of expected outcomes.
Comorbidity ScreeningComprehensive Medical Assessment
Cervical spine surgery carries specific risks related to various body systems. Thorough screening identifies conditions that increase surgical risk and allows optimisation before surgery.

Cardiovascular Assessment
Screening Questions
Key Considerations
- Low risk: No cardiac history, normal exam, good functional capacity
- Intermediate risk: Controlled HTN, prior MI >5 years ago, controlled AFib
- High risk: Recent MI (<6 months), unstable angina, decompensated heart failure
Management
- Cardiology referral if acute cardiac symptoms
- Recent MI or intervention requires clearance
- Significant arrhythmias need evaluation
Goal of Screening
Identify conditions that increase risk and allow optimisation before surgery—not to deny surgery but to improve safety.
Baseline Testing
Metabolic panel, coagulation studies, and specific tests as indicated form the pre-operative baseline for comparison.
Multidisciplinary Team CollaborationExpert Network Around You
Your preoperative assessment involves a coordinated team of specialists working together. Each brings unique expertise to ensure comprehensive evaluation and optimal outcomes.

Spine Surgeon
Team Leader
Responsibilities
Multidisciplinary Rounds Benefits
- Diverse expert input reduces individual bias
- Better risk stratification through multiple perspectives
- Improved patient education with team consensus
- Complex cases receive comprehensive evaluation
- Recommendations documented for clinical continuity
Specialist Consultations
Diagnostic Decision-MakingFrom Symptoms to Surgical Planning
The path from initial presentation to surgical decision follows a systematic algorithm. Clinical correlation—matching symptoms, imaging, and neurophysiological findings—is essential for optimal outcomes.
Diagnostic Algorithm
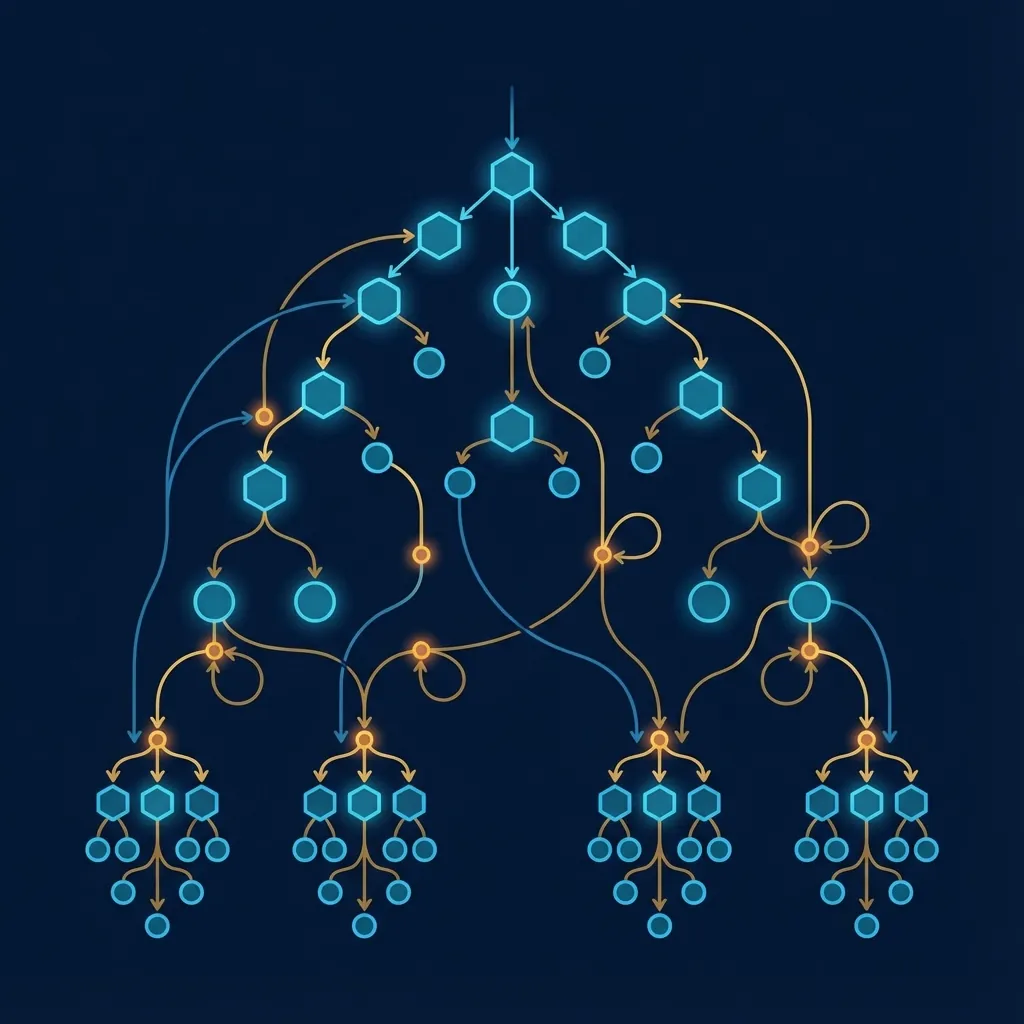
Patient presents with neck pain ± arm pain
History, physical exam, red flag screening
Red flags identified?
No → Conservative care trial (6–12 weeks) | Yes → Urgent imaging
Conservative care fails or red flags present
MRI cervical spine (first-line imaging)
MRI shows surgically relevant pathology
CT cervical spine (bone anatomy detail)
Clinical Correlation Examples
Symptoms
- Thumb/index finger pain radiating from neck
- Thumb numbness
- Wrist extension weakness
Imaging Findings
- C5-C6 right-sided herniation
- Compressing right C6 root in foramen
EMG/NCS (if performed)
- Right C6 paraspinal fibrillations
- Abnormalities in musculocutaneous and median nerve territories (C6 muscles)
Clinical Correlation
Perfect symptom-imaging-EMG correlation
Surgical Planning
C5-C6 anterior discectomy, placement of cervical disc prosthesis
Key insight: Imaging findings alone don't determine surgery. The correlation between symptoms, examination, imaging, and neurophysiological testing guides the optimal treatment plan.
Shared Decision-MakingYour Voice in Your Care
Surgery is a partnership. Your surgeon provides expertise, evidence, and recommendations. You provide your values, preferences, and goals. Together, you reach a truly informed decision.
Evidence-Based Discussion

Outcome Statistics
Valid Informed Consent Requires
- Patient understands nature and purpose of surgery
- Patient understands realistic alternatives (conservative care, fusion, arthroplasty)
- Patient understands material risks (infection, nerve injury, vascular injury, etc.)
- Patient understands likely benefits (pain relief, neurological improvement)
- Patient's decision is voluntary (no coercion)
- Patient has opportunity to ask questions
Consent Process
- 1Surgeon explains in understandable language (not jargon)
- 2Patient asks questions (encouraged)
- 3Surgeon clarifies any concerns
- 4Patient signs formal consent document
- 5Documentation in medical record
Risks to Discuss
Your Questions Are Welcome
Take time to understand your options. Write down questions before your consultation. There is no such thing as a "silly" question when it comes to surgery on your spine. Your surgeon wants you to feel confident and informed.
Preoperative OptimisationPreparing Your Body for Surgery
The weeks before surgery are an opportunity to optimise your body for the best possible outcomes. Each area of preparation contributes to faster recovery, fewer complications, and better long-term results.

Physical Therapy & Conditioning
Why It Matters
Recommendations
- Cervical spine stabilisation exercises
- Upper extremity strengthening
- Postural training
- Range of motion preservation
- Education on proper lifting, ergonomics
Your Role in Optimisation
Active participation in preoperative optimisation is one of the most important things you can do to influence your surgical outcome.
Medication List Essential
Bring a complete list of all medications (including supplements) to your preoperative visit for review and planning.
Advanced Surgical PlanningYour Unique Anatomy, Precisely Mapped
Modern imaging technology allows your surgeon to create patient-specific surgical plans based on your exact anatomy. This precision planning translates to better outcomes and reduced surgical time.

3D Reconstruction
Patient-specific 3D models generated from CT data for precise anatomical understanding.
Clinical Benefits
- Visualise your unique anatomy before surgery
- Identify unusual structures or variations
- Plan optimal approach trajectory
Anatomical Variants Requiring Recognition
Implant Selection Strategy
Disc Space Dimensions
Length, width, height measured on imaging; implant sized to fit
Endplate Geometry
Flat vs. lordotic implants chosen based on segmental anatomy and lordosis needs
Implant Material
Metal-on-plastic, metal-on-metal, or other bearing surfaces based on patient factors
Surgeon Familiarity
Experience with specific implants is important for optimal outcomes
Institutional Protocols
Hospital often standardises on 1–2 implant systems for consistency
Final sizing is typically done intraoperatively after disc removal and endplate preparation, but preoperative planning narrows options and aids surgical efficiency.
Assessment for OutcomesThe Foundation of Outstanding Surgery
Preoperative assessment is the foundation of excellent surgery. Every element—history, examination, imaging, neurophysiological testing, specialist input, shared decision-making, and optimisation—contributes to achieving the best possible outcomes.

Patient Safety
Identifies and optimises medical conditions that increase surgical risk
Surgical Technique
Detailed imaging, testing, and clinical correlation optimise approach and implant positioning
Outcome Optimisation
Appropriate patient selection, careful technique, realistic expectations lead to better outcomes
Patient Confidence
Thorough evaluation demonstrates thoroughness and builds confidence in surgical team
Legal/Ethical Standards
Informed consent ensures ethical practice and informed decision-making
Assessment Transforms Outcomes
Patients with excellent preoperative assessment typically experience:
Your Role in Assessment
As a patient, you contribute by:
- Providing honest symptom history
Accurate timeline, location, functional impact
- Communicating medical history
All prior surgeries, medical conditions, medications, allergies
- Asking questions
Understanding the plan and risks
- Following preoperative instructions
NPO, medications, arrival time
- Participating in optimisation
Smoking cessation, physical therapy, weight management if applicable
- Setting realistic expectations
Understanding recovery timeline and early postoperative course
Final Thoughts
By participating actively in your preoperative assessment, you ensure that you and your surgical team have the information needed to make the best possible decisions about your spine health and surgical care.
"Understanding your preoperative assessment process—including the important role of neurophysiological testing—transforms you from a passive patient into an informed partner in your own healthcare. This partnership, built on thorough assessment and clear communication, is the foundation for excellent surgical outcomes."