
Cervical Disc Replacement Neck Specialist
Revolutionary cervical arthroplasty procedures that preserve natural neck movement while eliminating pain and neurological symptoms. Internationally trained expertise ensures optimal outcomes using TGA-approved implants and evidence-based multidisciplinary care.
Success Rate
Evidence-Based Outcomes
98%
98% patient satisfaction rate with cervical disc replacement, validated through comprehensive long-term outcome measures and international clinical studies.
Years Experience
International Training
15+
Over 15 years of international fellowship training and experience in cervical motion-preserving surgery with expertise in complex multi-level procedures.
Motion Preserved
Full Range Restored
Natural
Complete preservation of natural cervical spine movement with restored range of motion, allowing return to normal activities without restriction.
Motion-Preserving Treatmentfor Degenerative Cervical Spine Disease
Cervical disc degeneration is one of the most common causes of chronic neck pain and arm symptoms in adults. For decades, the standard surgical treatment has been anterior cervical discectomy and fusion (ACDF)—a procedure that removes the diseased disc and permanently fuses the vertebrae together. This approach effectively resolves pain and neurological symptoms but comes with a long-term consequence: loss of motion at that level and accelerated degeneration at adjacent segments.
Cervical disc arthroplasty represents a fundamentally different strategy. Rather than eliminating motion through fusion, modern artificial disc implants replace the degenerated disc whilst preserving your cervical spine's natural biomechanics.

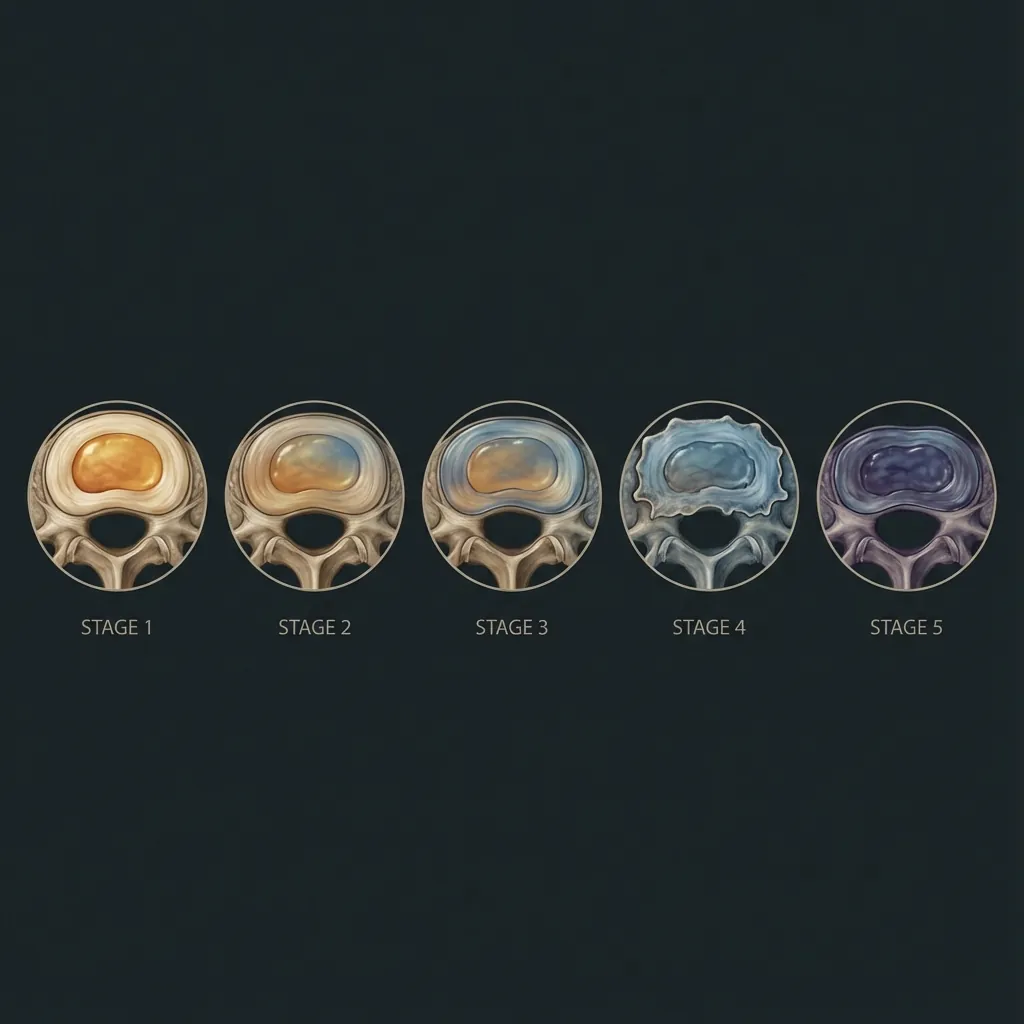
Why Cervical Discs Degenerate
Your cervical spine (neck) is a remarkably engineered structure consisting of seven vertebrae (C1–C7) separated by six intervertebral discs. These discs serve multiple critical functions: they absorb shock from daily activities, allow motion (flexion, extension, rotation, lateral bending), and maintain proper spacing between vertebrae so nerve roots can exit without compression.
The Natural Ageing Process Affects Discs
Through multiple mechanisms that compound over time:
Cervical Spine Structure
From Degeneration to Symptoms
Not All Degeneration Causes Symptoms
Many people have significant imaging findings (MRI changes, osteophytes, disc height loss) yet experience no pain or neurological symptoms. This is actually quite common—studies show that 25–50% of people without any neck pain have some degree of cervical disc degeneration visible on imaging.
Symptoms develop when the degenerated disc compresses structures that cause pain or neurological dysfunction. The three main clinical presentations are:

Occurs when the degenerated disc or osteophytes compress a nerve root as it exits the spine.
- Arm pain (often sharp, burning, or electric-like)
- Weakness in specific arm muscles supplied by that nerve root
- Numbness or tingling in the forearm or hand
- Pain typically radiates from the neck down into the shoulder, arm, and sometimes hand
Pain localised to the neck without arm symptoms can result from several mechanisms:
- Inflammation within the degenerated disc itself
- Facet joint arthritis from loss of disc space
- Muscle strain and spasm from altered biomechanics
- Internal disruption of the disc's architecture
The most serious presentation, occurring when significant disc herniation, osteophytes, or ligament thickening compresses the spinal cord itself:
- Weakness or clumsiness in hands
- Difficulty with fine motor tasks (writing, buttoning, eating)
- Leg weakness or stiffness (sometimes "rubber leg" sensation)
- Loss of balance or coordination
- Neck pain may be present or absent
- Myelopathy is a relative urgency and typically warrants surgery relatively soon after diagnosis
Myelopathy represents spinal cord compression and typically warrants prompt surgical evaluation to prevent permanent neurological damage.
What Is Cervical Arthroplasty?The Motion Preservation Principle
Cervical arthroplasty is a surgical procedure where the degenerated intervertebral disc is completely removed and replaced with a sophisticated artificial implant designed to preserve your spine's natural movement.
Restore Normal Disc Height
Opening the neural foramina to relieve nerve compression
Preserve Segmental Motion
Maintaining natural flexion, extension, and rotation at that spinal level
Distribute Loading
Sharing compressive forces across the vertebral bodies (as a natural disc does)
Maintain Spinal Biomechanics
Preventing the compensatory stress that develops after fusion
The Essential Difference from Fusion
Cervical Fusion (ACDF)
Traditional approach
When fusion is performed, the two vertebrae are permanently joined together with bone graft and often metal hardware. The fused segment becomes completely rigid.
Cervical Arthroplasty
Motion-preserving approach
Arthroplasty takes a different approach: rather than eliminating motion, it maintains motion using a mechanical device that replicates the disc's normal function.
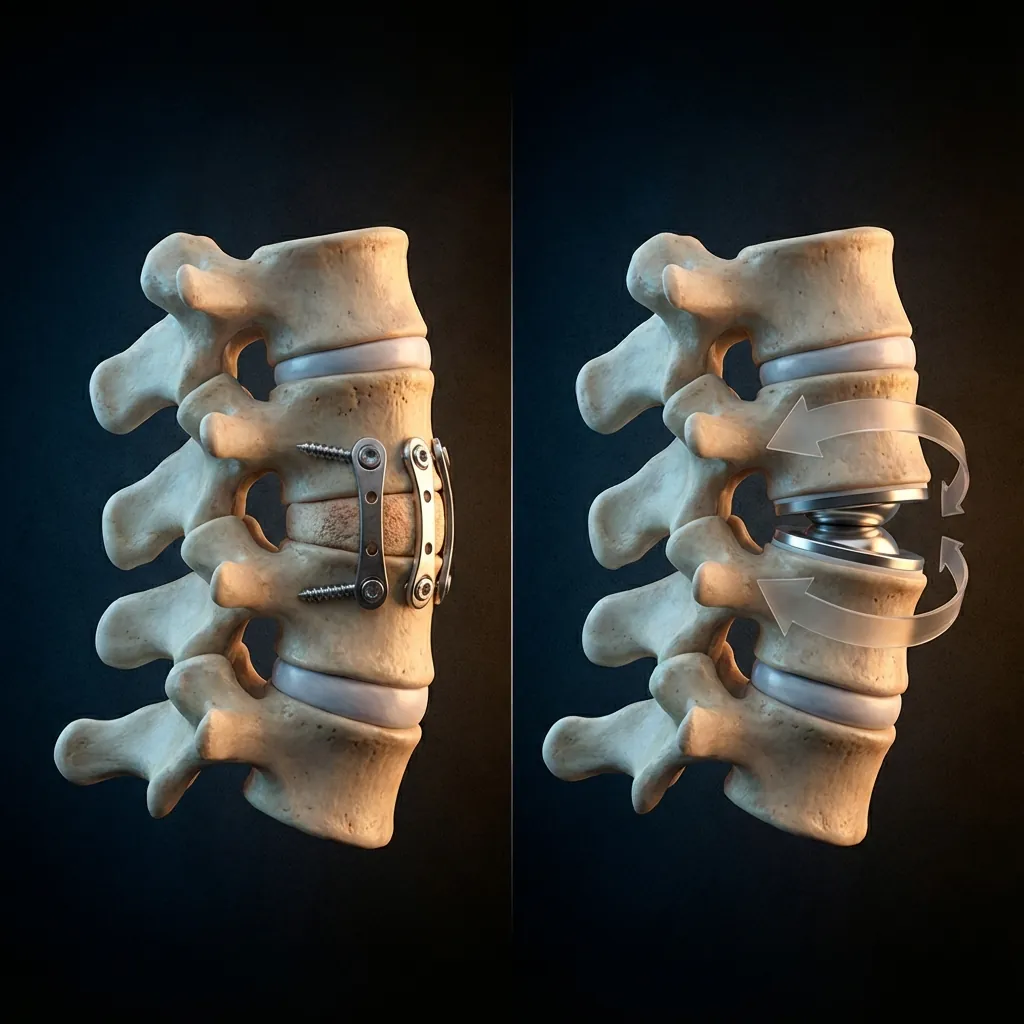
Motion preservation honours your spine's remarkable engineering and protects long-term spinal health
How Modern Cervical Artificial Discs Work
Modern cervical implants are engineering marvels—the result of over 20 years of biomechanical research and iterative design improvement. These devices must meet exacting requirements:

Anatomy Accommodation
Modern designs come in multiple heights, sagittal angles, coronal positions, and articulation types to match individual patient anatomy.
Available Implant Technologies
Ball-and-Socket Designs
e.g., ProDisc-C VIVO, Prestige LP
Feature a rounded convex surface on one endplate articulating against a concave surface on the other, allowing motion in multiple planes.
Each design has advocates, and outcome data is generally comparable across devices. The choice of implant depends on patient anatomy, surgeon preference, and specific biomechanical considerations for individual cases.
Why Choose Cervical Arthroplasty?Clinical Advantages Over Fusion
The medical literature comparing cervical arthroplasty with fusion demonstrates several consistent advantages for appropriately selected patients. These data come from prospective randomised controlled trials—the highest level of evidence.
The Problem with Fusion
- Adjacent-segment disease (ASD) develops in 25–35% of patients within 10 years
- Some require reoperation to address the new problem
The Arthroplasty Advantage
- ASD rates reduced to 10–15% at 10 years
- 50–67% reduction in risk compared to fusion
Why This Matters: If you're 50 years old undergoing cervical surgery, you have potentially 40+ years remaining. Protecting your adjacent segments now means fewer future surgeries and better spinal health across your entire lifetime.
Fusion Reoperation Data
- Approximately 9–15% require reoperation within 5–10 years
- Most often for new adjacent-level disease requiring fusion extension
Arthroplasty Reoperation Data
- Reoperation rates of 1–7% at 5–10 year follow-up
- National database: 1.24% at 5 years vs 9.23% for fusion
Why This Matters: Analysis of over 30,000 patients from a national insurance database confirms significantly lower reoperation rates with arthroplasty.
Fusion Results
- Zero motion at fused segment (by design)
- Global cervical motion reduced by 20–40%
Arthroplasty Results
- 85–90% of normal motion at operated level maintained at 10+ years
- Global cervical motion preserved at 70–80% of baseline
Why This Matters: Patients report better neck mobility, less stiffness, and better functional outcomes. The ability to rotate and bend your neck normally impacts quality of life, particularly for activities like driving, sports, and occupational demands.
Cervical Fusion Timeline
- Return to light work: 6–8 weeks
- Return to normal work: 12–16 weeks
- Full activity resumption: 4–6 months
Cervical Arthroplasty Timeline
- Return to light work: 4–6 weeks
- Return to normal work: 8–12 weeks
- Full activity resumption: 3–4 months
Why This Matters: The faster recovery reflects less tissue disruption with arthroplasty and the fact that fusion requires bone healing (bony union) which takes months.
Fusion 10-Year Data
- Composite success rate: 22–60%
- Adjacent-segment surgery: 15–25%
- Patient satisfaction: 70–85%
Arthroplasty 10-Year Data
- Composite success rate: 62–80%
- Adjacent-segment surgery: 3–5%
- Patient satisfaction: 80–90%
Why This Matters: Patients who improve after arthroplasty maintain their improvements at 10, 15, and even 20-year follow-up. There's no evidence of progressive deterioration of outcomes over time.
Who Is a Suitable Candidate?
Cervical arthroplasty offers excellent outcomes for appropriately selected patients. The assessment determines whether arthroplasty or fusion will provide the best long-term results for your specific situation.
Ideal Candidates
You are likely an excellent candidate if you have:
Relative Contraindications
Fusion may be more appropriate if you have:
Individual Assessment Is Essential
These criteria are guidelines, not absolute rules. Your surgeon will assess your specific anatomy, symptoms, imaging findings, and overall health to determine whether cervical arthroplasty or fusion will provide the best outcome for your individual situation.
Conservative Treatment Requirements
Before considering cervical arthroplasty, you should have exhausted reasonable conservative options. The goal isn't to make you try everything indefinitely, but rather to ensure you've given appropriate non-operative treatment a genuine chance before proceeding with surgery.

Rest and Activity Modification
Avoiding aggravating activities
Physical Therapy
Neck strengthening, postural education, flexibility exercises
Medications
NSAIDs, acetaminophen, muscle relaxants as appropriate
Lifestyle Modifications
Ergonomic adjustments, stress management
Interventional Procedures
Cervical epidural steroid injections or nerve root blocks (for appropriate patients)
Formal Physiotherapy Trial
Typically 6–12 weeks with qualified physical therapist
Most patients appropriate for surgery will have engaged in this conservative pathway. This ensures that surgery is reserved for those who genuinely need it and are likely to benefit from the intervention.
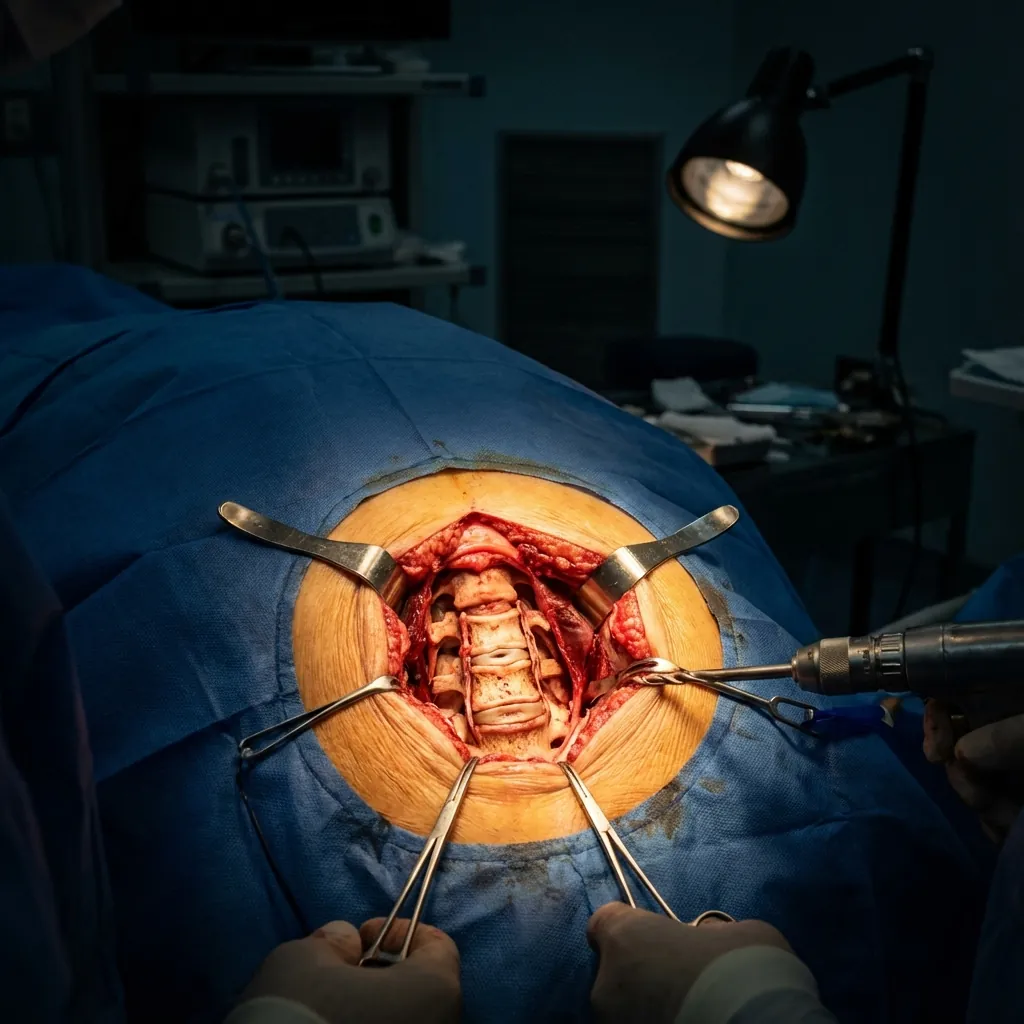
Surgical Technique and Procedure
Positioning: Supine (on your back) with slight neck extension to open the disc space
Incision: Small transverse incision (3–4 cm) along a natural neck crease, typically at the level of the cricoid cartilage
Approach: Anterior cervical approach—we develop a plane between the sternocleidomastoid muscle (laterally) and the visceral structures (trachea, oesophagus—medially), providing direct access to the cervical spine's anterior surface.
Preoperative Preparation
Before your surgery, you'll undergo:
Step-by-Step Surgical Steps
What You'll Experience Immediately After Surgery
In recovery
You'll wake in the recovery room under observation for 2–4 hours. Pain will be managed with intravenous medications.
Hospital stay
Depending on surgeon preference and your condition, you may go home the same day or stay overnight.
Initial pain
Expect significant incision pain for the first few days (typical 7–9/10), which is normal and managed with medications.
Neck stiffness
Your neck will feel very stiff and limited in motion—this is normal due to swelling and muscle guarding.
Swallowing
Temporary mild difficulty swallowing is common and usually resolves within days to weeks.
Recovery Timeline and Milestones
Recovery follows a predictable pattern with five distinct phases. Understanding what to expect at each stage helps you prepare for the journey ahead.
Immediate Postoperative
7–9/10 (incision pain dominant)
Bed rest with minimal movement; bathroom only with assistance
Minimal; neck feels locked and extremely stiff
Narcotic pain medications (oxycodone, hydromorphone) every 4–6 hours
Absolutely not—narcotic medications impair reflexes
Impossible; focus on recovery
Realistic Recovery Expectations
What WILL Improve
What Typically Does NOT Become Perfect
Long-Term Outcomes—The Evidence
The most important question patients ask: "Will this actually work long-term, or will I eventually need more surgery?"
Recent prospective randomised trials and large registry studies provide reassuring answers.
10-Year Follow-Up Data
Patient-Reported Outcomes
Reoperation Rates
Motion Preservation
Radiographic Findings
Comparison with Cervical Fusion at 10 Years
| Outcome (10-Year Follow-Up) | Cervical Arthroplasty | Cervical Fusion |
|---|---|---|
| Composite Success | 62–80% | 22–60% |
| Reoperation Rate | 7–10% | 20–30% |
| Adjacent-Level Surgery | 3–5% | 15–25% |
| NDI Improvement | 60–75% | 50–70% |
| Patient Satisfaction | 80–90% | 70–85% |
| Cervical Motion Preserved | 70–80% | 10–30% |
Key Finding: The reoperation advantage favouring arthroplasty becomes increasingly pronounced at longer follow-up, with the cumulative difference substantial by 10 years.
20-Year Data (Recently Published)
In 2023, the first 20-year follow-up data from the original FDA trial was published. Findings:
Motion maintained
82% of cervical arthroplasty patients had functional motion at 20 years
Superior to fusion
Global cervical motion significantly greater in arthroplasty group (47.8° vs 33.4°)
Adjacent-segment protection
Significantly lower adjacent-segment degeneration in arthroplasty group
Durability confirmed
No implant failures or major implant-related complications
Common Concerns—Honest Answers
We believe in transparent communication. Here are direct answers to the questions patients most frequently ask about cervical disc replacement.
Modern cervical disc implants are designed to last decades. Long-term clinical studies show no evidence of implant failure due to wear or material breakdown. The materials used (titanium alloy, cobalt-chrome, polyethylene) are proven in other orthopaedic applications (hip replacements) where they function for 15–20+ years reliably.
- The cervical spine experiences significantly less force and fewer repetitive cycles than the hip joint
- A hip joint might experience millions of loading cycles annually; the cervical spine experiences hundreds of thousands
- This reduced stress means substantially less wear
Bottom line: Expect your cervical disc implant to function reliably for your remaining life. While distant future technology might eventually require revision, this is not a foreseeable concern.
Some cervical disc implants do contain metal components that might trigger security scanners, particularly sensitive airport security. However, you'll receive an implant identification card that you can show to security personnel, explaining that you have a cervical implant.
- Modern security systems are generally designed to accommodate people with metal implants
- Airport TSA personnel are trained to handle patients with implants
- You may be subject to additional screening (pat-down, swab) but passage is not prevented
Bottom line: Your implant won't prevent travel, though you may experience minor additional security screening in some airports. The identification card resolves most situations.
Yes, modern cervical disc implants are MRI-compatible. You can safely undergo MRI imaging for diagnostic purposes.
- The metallic components of your implant may produce some artifacts (image distortion) on the MRI, particularly in the immediate vicinity of the implant
- This rarely prevents diagnosis but should be communicated to your radiologist
- More distant areas (brain, lumbar spine) image normally
- Alert the MRI facility to your implant—they'll verify specific implant model compatibility and may adjust scanning protocols accordingly
Bottom line: MRI is safe and available to you; you simply need to inform the facility of your implant.
Cervical arthroplasty does not prevent future spine procedures if they become necessary. The implant can be revised if needed (though this is exceptionally rare), and additional levels can be addressed with either arthroplasty or fusion at adjacent segments.
- Because arthroplasty reduces adjacent-segment disease risk by 50–67%, you're less likely to need future surgery at adjacent levels compared to fusion patients
- If you develop new symptomatic disease at a different level (e.g., C4–C5 arthroplasty now, new C3–C4 disease later), you could undergo a second arthroplasty at the new level
- If two-level fusion is eventually indicated, this is technically feasible even with a prior arthroplasty
Bottom line: Cervical arthroplasty doesn't burn bridges for future treatment. It actually reduces the need for future surgery by protecting adjacent segments.
This comparison is addressed in detail throughout this page, but briefly:
- Arthroplasty advantages: Better long-term motion preservation, lower adjacent-segment disease risk, lower reoperation rates, faster recovery, better patient satisfaction in most series
- Fusion advantages: More predictable immediate stability, longer track record (fusion has been done for 60+ years), potentially simpler surgery, sometimes preferred for specific anatomy
Bottom line: For appropriately selected patients (single or two-level disc disease with adequate bone quality), cervical arthroplasty demonstrates superior long-term outcomes compared to fusion. However, for specific anatomical situations (severe facet disease, kyphosis, osteoporosis), fusion may still be preferred.
Decision-Making Framework
Understanding when surgery is indicated and how to choose between arthroplasty and fusion requires careful consideration of multiple factors.
When Is Surgery Indicated?
Conservative care has been tried genuinely (6–12 weeks of structured physiotherapy and medical management) AND you have one or both of these:
Persistent symptoms significantly limiting quality of life
Pain or neurological symptoms severely restricting work, activities, or causing substantial suffering despite conservative care
Progressive neurological deficit
Worsening weakness, spreading numbness, or myelopathic signs despite conservative care (this is a relative urgency)
How to Decide Between Arthroplasty and Fusion?
This conversation with your surgeon should explore:
Does your imaging show features suggesting arthroplasty (preserved disc height, minimal facet disease, adequate bone quality) or suggesting fusion (severe facet disease, marked kyphosis, osteoporosis)?
How important to you is preserving neck motion? Do you have occupational or lifestyle activities that benefit from preserved motion? This is a valid reason to choose arthroplasty.
If you're 45 years old with good health expecting 50+ years remaining, adjacent-segment disease protection becomes more valuable. If you're 75 with other health limitations, this matters less.
Has your surgeon performed many arthroplasties? Is he/she experienced with both approaches? Outcomes are better with surgeon experience.
Arthroplasty has slightly lower overall complication and reoperation rates but requires more precise surgical technique. Fusion is more forgiving technically but has higher long-term reoperation rates.
Navigating the Detailed Resources
From this introduction, you can explore six detailed resource pages for deeper understanding of specific topics.
Cervical Anatomy
Understanding normal cervical spine structure, intervertebral discs, nerve roots, and how degeneration develops.
Cervical History
Historical development of cervical arthroplasty, evolution from fusion to motion-preserving approaches, key clinical trials.
Preoperative Assessment
Detailed explanation of imaging findings, what your MRI shows, how diagnosis is confirmed, preparations for surgery.
Cervical Implants
In-depth review of currently available implant designs, biomechanical characteristics, how implants are selected for individual patients.
Surgical Technique
Comprehensive step-by-step surgical walkthrough with detailed descriptions of each operative stage.
Cervical Recovery
Detailed recovery timeline, rehabilitation protocol, when specific activities resume, managing recovery challenges.
Download Your GuidesCervical Disc Replacement
Free, evidence-based patient guides covering every stage of your cervical disc replacement journey — from initial assessment through long-term recovery.
Cervical Disc Replacement Guide
Complete patient guide to cervical arthroplasty — indications, procedure, recovery, and outcomes.
Pre-Operative Preparation
Everything you need to prepare for your cervical disc replacement surgery.
Post-Operative Recovery
Step-by-step recovery milestones, restrictions, and return-to-activity timelines.
Exercise & Rehabilitation
Structured rehabilitation programme with progressive exercises for cervical recovery.
Medicare & Insurance Guide
Understanding Medicare item numbers, private health insurance, and cost transparency.
Looking for more resources?
Visit the full Patient Resources library for all available guides, including long-term wellness, return to sport, and decision-making frameworks.
Explore Cervical Disc Replacement In Depth
Each topic below takes you deeper into the cervical disc replacement journey — from anatomy through surgical technique to recovery.
Cervical Spine Anatomy
Understand the seven cervical vertebrae, intervertebral discs, nerve roots, and spinal cord — the foundation for understanding disc disease.
Preoperative Assessment
Patient selection criteria, imaging requirements, and the comprehensive evaluation process used to determine surgical suitability.
Implant Technology
Explore the artificial disc designs available for cervical replacement — materials, biomechanics, motion characteristics, and longevity data.
Surgical Technique
Step-by-step walkthrough of the anterior cervical approach, discectomy, endplate preparation, and implant insertion.
Postoperative Care & Recovery
Recovery milestones from day 1 to 12 months — activity restrictions, physiotherapy, return to work, and long-term follow-up.
Long-Term Outcomes
10–20 year clinical data on pain relief, neurological recovery, motion preservation, and reoperation rates versus fusion.
Is Cervical Disc Replacement Right for You?

The Pinnacle of Motion-Preserving Spine Surgery
Cervical disc arthroplasty represents the pinnacle of motion-preserving spine surgery, combining sophisticated engineering, decades of clinical research, and proven long-term outcomes. For appropriately selected patients—those with single or two-level degenerative disc disease, adequate bone quality, and realistic expectations—cervical arthroplasty often delivers superior outcomes compared to traditional fusion.
The Central Principle
Rather than solving your current problem by creating permanent rigidity (fusion), arthroplasty solves your problem whilst honouring your spine's remarkable engineering and protecting your long-term spinal health.
Next Steps
Review your specific anatomy and diagnosis
Explore the Preoperative Assessment page
Understand surgical options
Compare arthroplasty technique versus fusion approach
Clarify your values
Consider what outcomes matter most to you
Discuss with your surgeon
Use the information here to engage in informed, collaborative decision-making
Prepare for consultation
Bring specific questions; request your surgeon's experience data
Remember: This information supports informed decision-making in partnership with your healthcare provider. Your personal situation, anatomy, and preferences should guide your final decision about whether cervical arthroplasty is right for you.