
Advanced Solutions Complex Conditions
When spinal pathology extends beyond single-level disease, advanced arthroplasty techniques offer solutions that preserve motion across multiple segments whilst addressing complex anatomical challenges. This comprehensive guide explores the frontier of motion-preserving spine surgery.
Adjacent-Segment Disease
Prevention Focus
ASD
Motion preservation strategies that reduce long-term degeneration risk at adjacent spinal levels.
Multilevel Arthroplasty
Complex Cases
2–4
Advanced techniques for treating degenerative changes spanning multiple spinal segments.
Strategic Approaches
Combined Solutions
Hybrid
Tailored combinations of motion preservation and fusion for optimal patient outcomes.
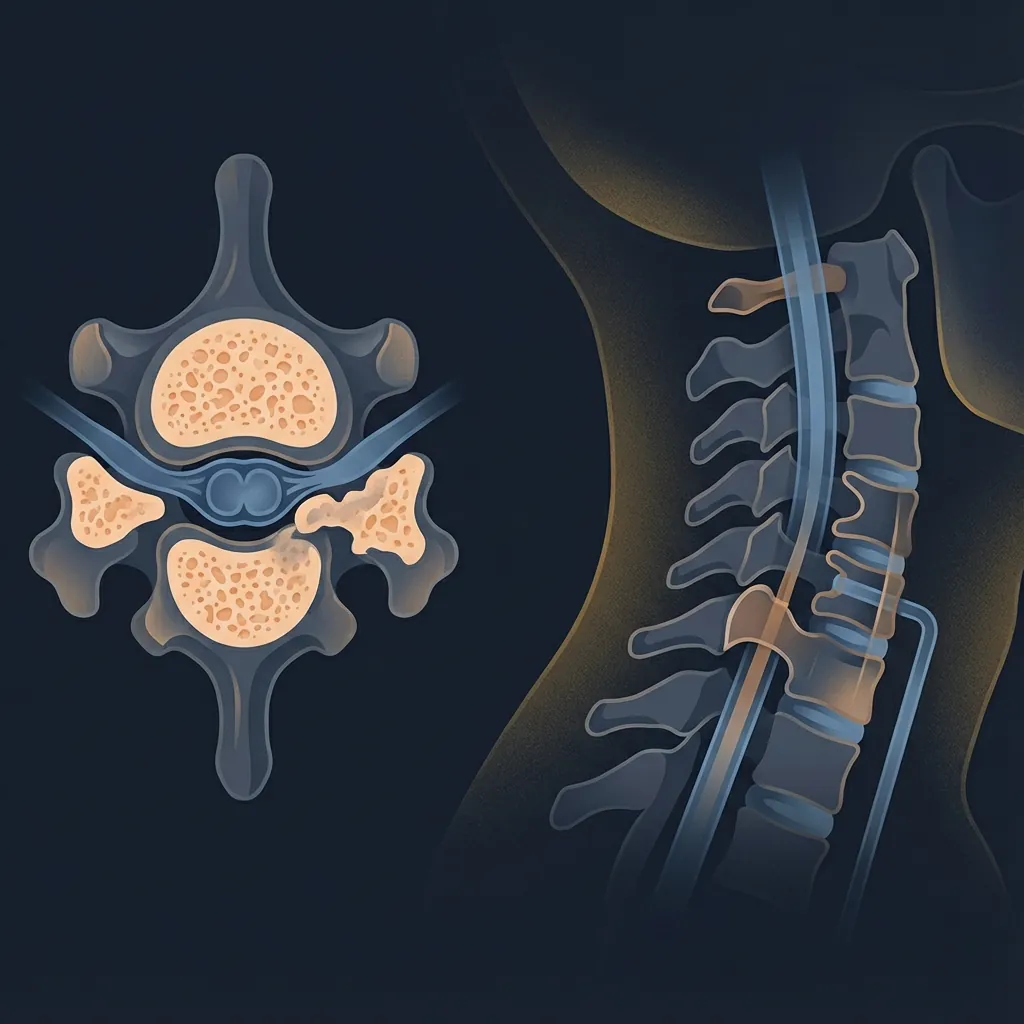
Understanding Adjacent-Segment Disease& Why Motion Preservation Matters
The fundamental problem with rigid fusion lies in altered biomechanics at spinal segments adjacent to the fused area. Rather than representing a 'solved' problem, fusion creates a new reality: complete elimination of motion at one level forces neighbouring segments to compensate by increasing their own motion.

The Biomechanical Cascade: How Fusion Creates Problems
Epidemiological Reality
Research findings demonstrate the clinical significance of adjacent-segment disease:
Cost and Morbidity Implications
The average cost of reoperation for adjacent-segment disease (including imaging, hospital stay, surgeon fees, implants, rehabilitation) ranges from $50,000–$100,000 AUD. Beyond financial cost, reoperation carries additional surgical risk (bleeding, infection, neurological injury) compounded by scarring from prior surgery.
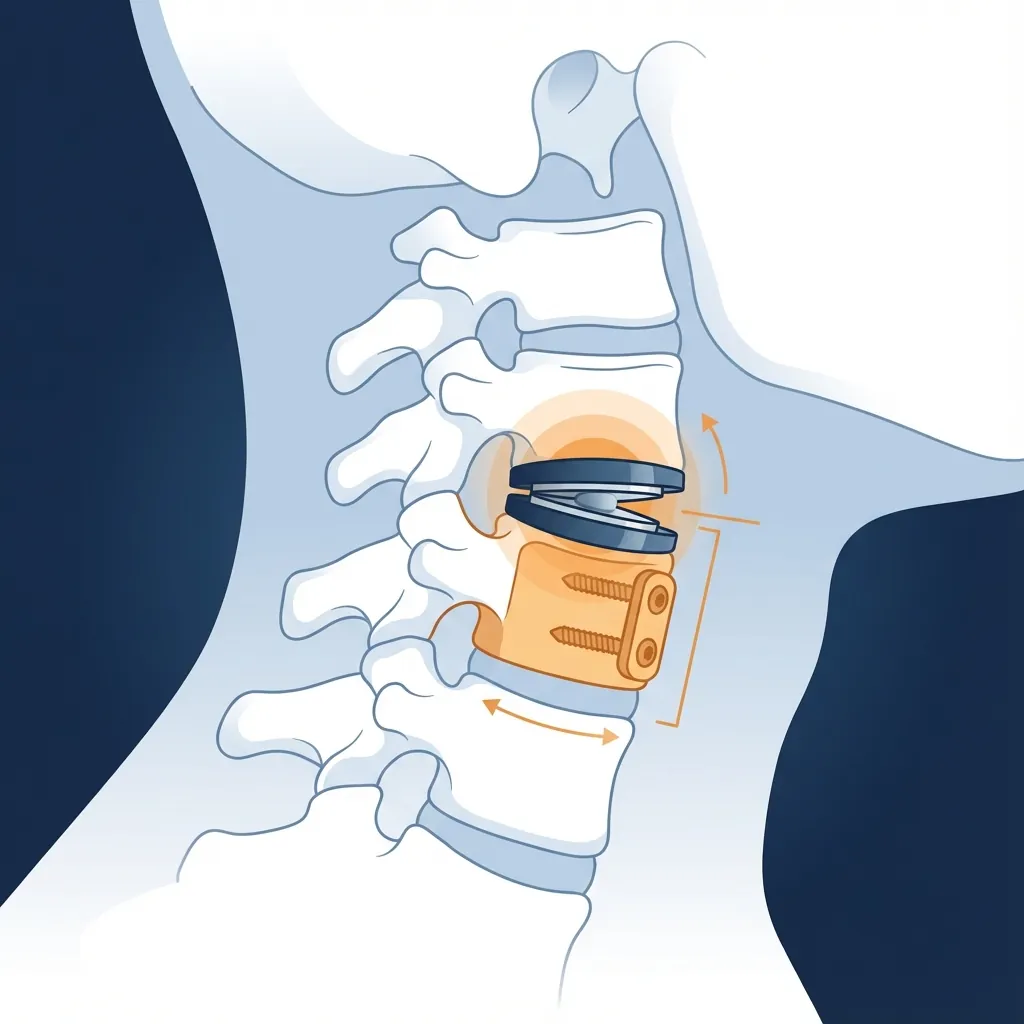
Motion Preservation: A Different Biomechanical Strategy
Cervical and lumbar arthroplasty represent a fundamentally different approach: Rather than eliminating motion at the diseased level, arthroplasty preserves segmental motion while eliminating pain through neural decompression and disc replacement.
How Motion Preservation Protects Adjacent Segments
Maintained Load Sharing
An artificial disc, like a natural disc, distributes compressive loads across the vertebral body endplates rather than concentrating them at posterior elements or shifting them to adjacent levels.
Preserved Motion Biomechanics
By maintaining normal or near-normal segmental motion, motion-preserving implants eliminate the compensatory motion mechanism that accelerates adjacent-segment degeneration.
Reduced Stress Concentration
Biomechanical studies using finite element analysis demonstrate that motion-preserving devices reduce peak stresses in adjacent segments by 20–40% compared to fusion constructs.
Extended Adjacent-Segment Survival
Clinical studies show that adjacent-segment disc height is better preserved, facet joint arthritis develops more slowly, and foraminal stenosis occurs less frequently after arthroplasty.
Evidence Quantifying the Adjacent-Segment Benefit
| Outcome | Arthroplasty | Fusion | Difference |
|---|---|---|---|
| Adjacent-segment degeneration (10 years) | 10–15% | 30–35% | 50–67% risk reduction |
| Reoperation for ASD (10 years) | 5–10% | 15–20% | 50–67% risk reduction |
| Patient satisfaction (10 years) | 85–90% | 75–80% | 10–15% advantage |
Strategic implication: For patients with significant life expectancy remaining (typically those <65–70 years with good health), the motion-preserving advantage becomes increasingly important across 20, 30, or 40 additional years of spinal function.
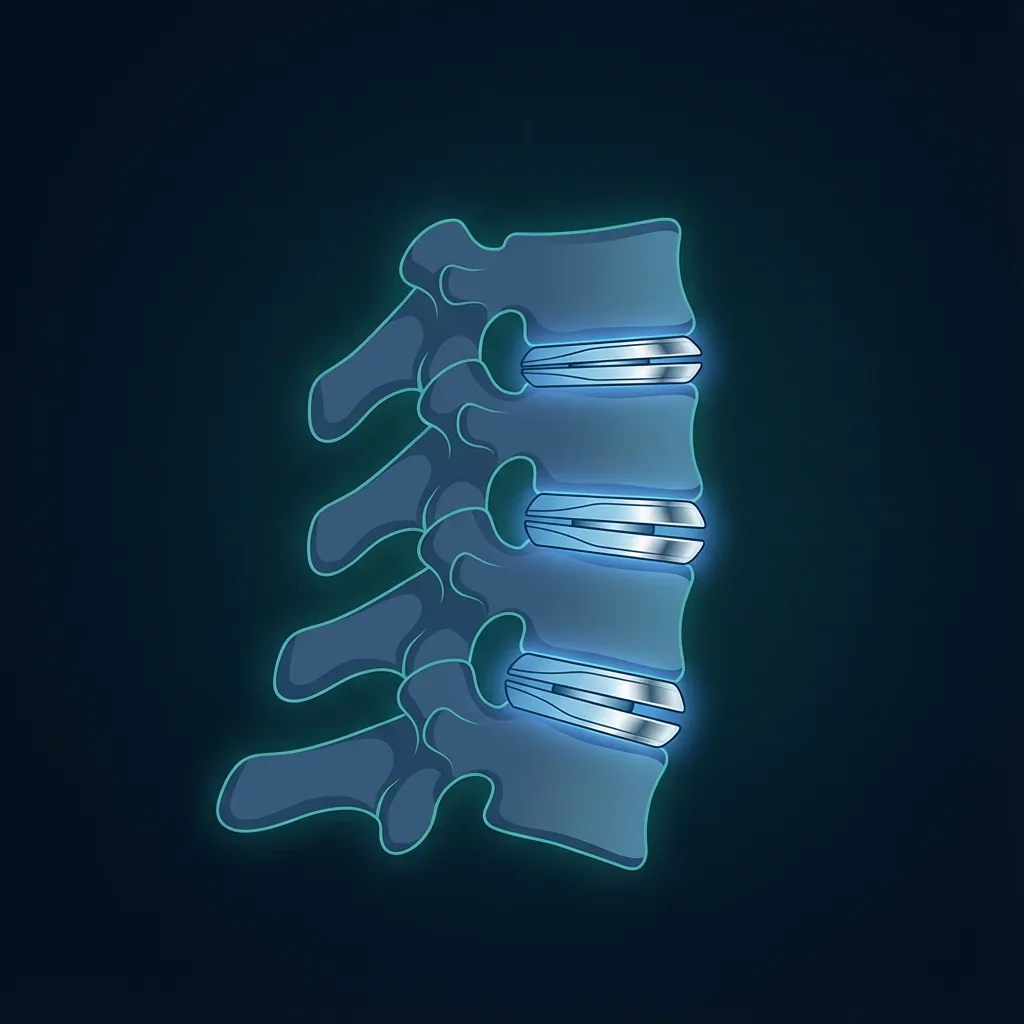
Multilevel ArthroplastyExtending Motion Preservation
Clinical Indications for Two-Level ACDA
Optimal scenarios include:
- Two adjacent levels with clear pathology (e.g., C5–C6 and C6–C7)
- Radiculopathy at both levels with imaging-clinical correlation
- Reasonable disc quality with adequate disc height and vertebral body quality
- Limited facet disease (Grade 0–2)
- No severe myelopathy (two-level myelopathy acceptable)
- Patient age typically <70 years with good health and life expectancy
- Demonstrated failure of conservative care
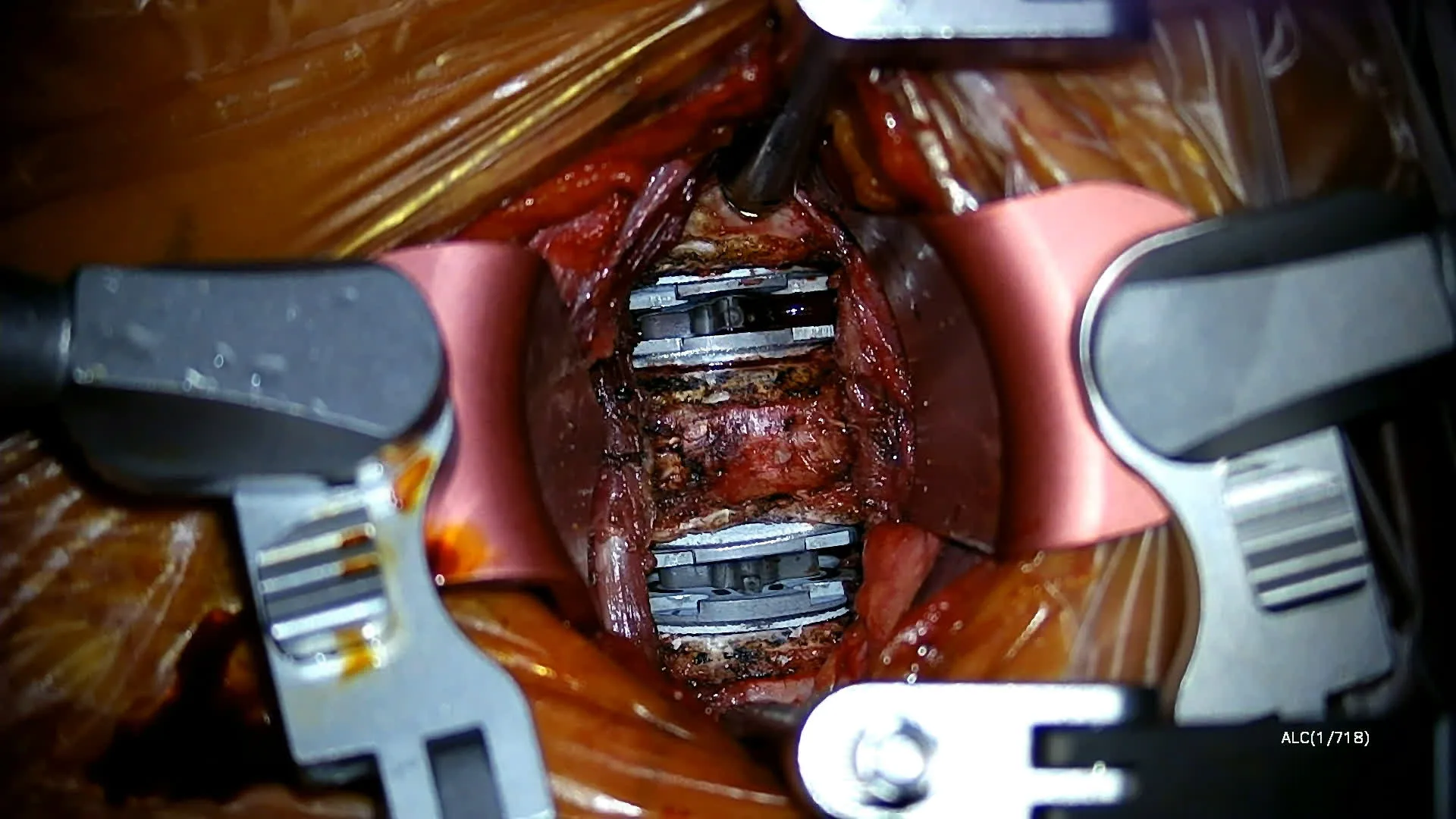
Surgical Considerations
Extended Operative Time
15–30 additional minutes compared to single-level, typically under 120 minutes total.
Implant Selection Consistency
Most surgeons use the same artificial disc design at both levels for biomechanical consistency.
Endplate Preparation
Careful preparation at both levels is critical; asymmetric preparation can compromise outcomes.
Fluoroscopic Confirmation
Each implant position verified independently with imaging.
Single Incision
Standard anterior approach typically accommodates two cervical levels.
Long-Term Outcome Data (7-Year Follow-Up)
Safety Profile
| Complication | Rate | Resolution |
|---|---|---|
| Dysphagia (temporary) | 10–20% | Resolves within 3–6 weeks; <1% persistent |
| Voice changes (temporary) | 5–10% | <1% persistent |
| Neurological complications | <1% | Exceptionally rare |
| Vascular complications | <1% | Rare |
| Subsidence | <5% | Usually asymptomatic |
| Heterotopic ossification | 10–20% | Rarely symptomatic |
When Three- or Four-Level ACDA Is Appropriate
Complex clinical scenarios include:
- Multilevel myelopathy: Cord compression at three or four cervical levels
- Multilevel radiculopathy: Symptomatic nerve compression at multiple levels
- Young patient with extensive disease (e.g., 45-year-old with life expectancy approaching 50 years)
- Failed conservative treatment of multilevel disease
- Patient preference for motion preservation (if technically feasible)
Crucial Selection Criteria
- Adequate vertebral body quality at all levels for implant fixation
- No severe kyphotic deformity (may require osteotomy instead)
- Limited facet disease (Grade 3–4 at multiple levels may contraindicate)
- Surgeon expertise with multilevel arthroplasty
- Realistic patient expectations about recovery and possible complications
Operative Strategy
Single-stage (all levels) vs staged approach (6+ weeks apart).
Most surgeons perform single-stage when patient health permits.
Operative Time
Three-level: 90–120 minutes
Four-level: 120–150 minutes
7-Year Follow-Up Data (139 Patients)
| Outcome | Preop | 3 Mo | 1 Yr | 7 Yrs |
|---|---|---|---|---|
| NDI Score | 57.9 | 35.2 | 30.1 | 31.3 |
| Neck Pain (NRS) | 15.6 | 8.1 | 7.2 | 7.9 |
| Arm Pain (NRS) | 12.2 | 5.8 | 4.9 | 5.6 |
| ROM (degrees) | 6.2 | 5.8 | 6.1 | 6 |
Interpretation: Significant improvement from baseline maintained at 7 years; segmental motion preserved at all three or four levels.
Two-level cervical disc replacement demonstrating motion preservation at C5–C6 and C6–C7
Clinical Superiority Demonstrated
Meta-analyses demonstrate two-level ACDA outcomes statistically superior to two-level fusion on multiple measures. The motion-preserving advantage extends across:
- Reduced adjacent-segment degeneration rates
- Lower reoperation rates at 10+ years
- Higher patient satisfaction scores
- Preservation of global cervical motion
Hybrid SurgeryStrategic Combination of Arthroplasty and Fusion
Hybrid surgery—the combination of cervical disc arthroplasty at certain levels with anterior cervical discectomy and fusion (ACDF) at other levels in the same patient—represents sophisticated surgical problem-solving.
Conceptual Foundation: Matching Technology to Pathology
Rather than applying single technology (arthroplasty everywhere or fusion everywhere), hybrid surgery applies each technology where it is most appropriate, based on:
Hybrid Patterns in Clinical Practice
Two-Level Hybrid Patterns
C5–C6 severe facet disease unsuitable for arthroplasty; C4–C5 ideal arthroplasty candidate
One mobile level preserved (C4–C5) reduces adjacent-segment risk vs two-level fusion
C4–C5 with severe myelopathy prefers fusion stability; C5–C6 amenable to arthroplasty
Motion preservation at lower level (higher risk for ASD due to L5–S1 proximity)
L4–L5 motion preservation desirable; L5–S1 may prefer fusion stability for sacral junction loading
Motion preserved at L4–L5 reducing L3–L4 risk; L5–S1 stabilised
Three-Level Hybrid Patterns
Middle level (C4–C5) has severe myelopathy or facet disease requiring fusion; flanking levels preserved
Two mobile segments preserved despite fusion at one level
Outcome Data for Hybrid Surgery
Comparative study data (meta-analysis 2016–2019): When hybrid surgery outcomes compared to three-level ACDF and three-level ACDA:
| Parameter | Hybrid Surgery | Three-Level ACDF | Three-Level ACDA |
|---|---|---|---|
| NDI Improvement | 48% | 42% | 52% |
| Total C2–C7 ROM (degrees) | 32.1 | 18.5 | 38.2 |
| Patient Satisfaction | 82% | 75% | 87% |
| Reoperation Rate | 8% | 18% | 10% |
| Dysphagia Rate | 12% | 20% | 15% |
Interpretation: Hybrid surgery achieves outcomes intermediate between pure fusion and pure arthroplasty, maintaining meaningful motion preservation while allowing strategic fusion where anatomy demands it.
Long-term data: Seven-year follow-up studies demonstrate sustained satisfaction (80%+) and low reoperation rates (8–12%).
Hybrid Surgery in Practice: Clinical Scenarios
Clinical Findings
- C4–C5: Moderate disc herniation, Grade 1 facet arthritis → ACDA suitable
- C5–C6: Large disc herniation, Grade 3 facet arthritis → Fusion preferred
- C6–C7: Moderate herniation, Grade 2 facet disease → ACDA suitable
Hybrid Approach
C4–C5 ACDA, C5–C6 ACDF, C6–C7 ACDA
Clinical Findings
- Prior L4–L5 fusion remains in place
- New L5–S1 disc herniation causing symptoms (adjacent-segment disease)
Hybrid Approach
Add L5–S1 ALDA (motion-preserving device) below existing fusion — do NOT extend fusion
Clinical Findings
- C5–C6: Unilateral right disc herniation with foraminal stenosis; excellent disc height, no facet disease
- C6–C7: Central disc bulge with mild bilateral foraminal stenosis; reduced disc height, Grade 2 facet arthritis
Hybrid Approach
C5–C6 ACDA (ideal candidate), C6–C7 ACDF (facet disease and reduced disc height less favourable)
Complex Anatomical ScenariosNavigating Challenging Clinical Situations
Strategic Considerations
Anterior Approach Safety
When accessing spine anterior to existing posterior fusion hardware, anterior approach remains safe. Posterior hardware does not interfere with anterior approach or disc replacement placement.
Vascular Adhesions
Primary concern with revision anterior approach is vascular adhesions from prior anterior approach. If prior fusion was posterior-only, adhesion risk minimal.
Implant Selection
Artificial disc placement adjacent to prior fusion is biomechanically sound—the implant at the mobile level compensates for motion loss at fused level.
Long-Term Outcomes
Published series demonstrate 85–90% satisfaction with arthroplasty placed adjacent to prior fusion, with reoperation rates (5–10%) similar to unfused spines.
Case Example: Extension Surgery After Prior Two-Level Fusion
Prior surgery: Two-level ACDF at C5–C6 and C6–C7 (8 years prior)
Current presentation: Symptomatic C4–C5 adjacent-segment disease with disc herniation and foraminal stenosis
Would create extensive construct with high adjacent-segment risk at C3–C4
Maintains motion at C4–C5; accepts fusion at C5–C7; distributes load better
Recommended ApproachOperationally complex but theoretically superior biomechanics
Contemporary Evidence
- Two major prospective trials demonstrate superior or non-inferior outcomes for ACDA vs. ACDF in myelopathy patients
- Meta-analysis data: Myelopathy resolution rates 80%+ in ACDA group comparable to ACDF group
- T2 hyperintensity (spinal cord signal change) resolves in majority of ACDA myelopathy patients
Key Selection Factors for Arthroplasty in Myelopathy
Technical Considerations in Myelopathy Surgery
- Intraoperative visualisation of cord before and after decompression (some use intraoperative ultrasound)
- Complete removal of all anterior pathology (disc, osteophytes) critical in myelopathy
- Some surgeons employ intraoperative neurophysiological monitoring (IONM)
- Meticulous haemostasis—epidural haematoma can compromise decompression gains
- Neurological recovery slower than radiculopathy: progressive improvement over 3–6 months
Arthroplasty-Specific Concerns
Endplate Fixation
Implant endplates rely on contact with vertebral bone. In severe osteoporosis, bone quality compromised and endplate purchase suboptimal.
Subsidence Risk
Implant may settle (subside) into vertebral body over time, potentially causing loss of disc height or kyphosis.
Implant Migration
Poor bone quality increases risk of implant shifting from intended position.
Current Evidence
Limited data on arthroplasty specifically in severe osteoporosis. Most trials excluded patients with T-score <–2.5. Published case series suggest feasibility but with higher subsidence rates (10–25%) compared to normal bone quality.
Management Strategies
- 1Preoperative optimisation: Address osteoporosis with medical therapy (bisphosphonates, vitamin D, calcium) for 3–6 months preoperatively if time permits
- 2Selective application: Reserve arthroplasty for cases where strong indication exists; fusion more conservative approach
- 3Augmentation techniques: Some surgeons use bone graft, bone cement, or augmentation techniques to improve endplate support
- 4Conservative implant selection: Some surgeons prefer larger-diameter implants offering greater surface area contact
Realistic Counsel: Patients with severe osteoporosis should understand that arthroplasty, while potentially beneficial, carries higher risk than in normal bone quality, and fusion may represent safer option.
Why Kyphosis Matters: Kyphotic alignment alters loading patterns, potentially reducing motion-preserving benefits and increasing adjacent-segment risk.
Approach by Severity
Loss of <20° lordosis from normal ~40°
ACDA with restoration of lordosis through implant positioning may be adequate
Significant kyphotic deformity
ACDA combined with osteotomy (bone removal and realignment) addresses both pathology and deformity—increases operative complexity
Kyphosis primary problem, neural compression secondary
Posterior deformity correction with instrumentation and fusion rather than anterior discectomy-arthroplasty
Long-Term Outcomes: Published series of ACDA with concurrent kyphosis correction demonstrate good outcomes with maintained motion and improved sagittal alignment.
Evidence SynthesisWhy Advanced Arthroplasty Works
The most compelling evidence for advanced arthroplasty comes from long-term follow-up studies tracking patients for 7, 10, and even 15+ years—demonstrating sustained benefits and remarkable device durability.

Long-Term Durability: The 10+ Year Picture
Ten-Year Cervical Arthroplasty Outcomes
Prospective randomised trials following >400 patients for 10 years (FDA IDE studies) demonstrate:
Clinical Comparison to Fusion
| Metric | Arthroplasty | Fusion | Note |
|---|---|---|---|
| Functional Improvement | Comparable | Comparable | Similar pain relief achieved |
| Adjacent-Segment Disease | 10–15% | 30–40% | Significantly lower with arthroplasty |
| Reoperation Rate | 5–10% | 15–25% | Lower with arthroplasty |
Why Device Durability Is Remarkable
Theoretical Concerns vs Clinical Reality
When arthroplasty was first introduced, orthopaedic surgeons raised concerns based on hip and knee replacement experience: wouldn't artificial discs undergo polyethylene wear, particle generation, and osteolysis? Clinical reality diverges from theory:
Ten-year imaging studies: Radiographic analysis of implants at 10 years shows stable position (no migration), maintained disc height (no subsidence), preserved motion, and no evidence of excessive wear or material degradation.
Patient Selection and Outcomes Relationship
Evidence clearly demonstrates that outcomes depend critically on appropriate patient selection.
Ideal Candidates: 90–95% Satisfaction
Age 40–65, clear imaging correlation, failed conservative care, no severe facet disease
Key Point: Poor outcomes in advanced arthroplasty typically reflect poor patient selection rather than procedural inadequacy.
Specialised Surgeon Skill Requirements
Advanced arthroplasty—especially multilevel, hybrid, and complex scenario cases—demands specific surgeon expertise beyond standard ACDF or simple arthroplasty skills.
Technical Skills
- Anterior cervical or lumbar approach expertise with appropriate vascular management
- Endplate preparation technique: precise depth, angulation, and symmetry
- Implant sizing and positioning for optimal biomechanics
- Intraoperative imaging proficiency to verify positions at multiple levels
- Problem-solving ability: recognise suboptimal positioning and adjust in real-time
- Vascular surgery collaboration: safe work around major vessels
Clinical Judgment
- Patient selection: appropriate filtering; recognising contraindications
- Multilevel decision-making: when to perform two-level vs. one-level with watchful waiting
- Hybrid strategy development: recognising when hybrid approach optimal
- Complication management: early recognition and appropriate management
Experience Metrics
- 100+ total arthroplasty cases before advancing to multilevel
- 50+ multilevel cases (two-level) before attempting three-level
- Ongoing participation in training, literature review, and case discussion
- Access to specialised equipment and instrumentation
- Facility support: experienced anaesthesia, neuromonitoring, vascular consultation
Decision-Making AlgorithmsFramework for Complex Cases
When evaluating a patient with multilevel spinal pathology, systematic assessment guides treatment selection through four critical steps.
Establish Which Levels Are Symptomatic
Not all degenerative findings require surgical treatment. Only symptomatic levels—where pathology correlates with patient's clinical presentation—should be addressed.
Assessment Method:
- Clinical history and examination localise patient's symptoms to specific dermatomal distributions or pain patterns
- Imaging identifies pathology at multiple levels
- Critical step: Correlate imaging to clinical presentation
- Example: Does the C6 nerve root compression match the patient's thumb pain?
- Example: Does the L5–S1 disc herniation match the patient's left leg symptoms?
Clinical Pearl: Treating asymptomatic/incidental degenerative findings increases operative complexity and reoperation risk without benefiting patient.
Patient CounsellingRealistic Expectations for Advanced Arthroplasty
Patients considering multilevel arthroplasty require thorough counselling about realistic expectations, benefits, and risks.
Recovery Timeline
Multilevel (two-level or more) procedures typically require:
Realistic Outcomes
Success definition: Rather than "cure," arthroplasty achieves:
Advantages
Significant pain relief (typically 70–85% reduction, not 100% elimination)
Functional restoration to near preoperative baseline or improved
Neurological improvement (reversal of radiculopathy/myelopathy symptoms)
Motion preservation demonstrated on imaging
Disadvantages
Complete pain elimination (residual mild discomfort common, typically 1–2/10)
Return to all pre-disease activities (some permanent limitations occasional)
Prevention of all future spine problems (adjacent-segment disease still possible, though reduced)
Complication Counselling
Temporary Complications (usually resolve)
| Complication | Rate |
|---|---|
| Dysphagia (difficulty swallowing)Mostly resolving within 6 weeks | 10–20% |
| Voice hoarsenessTemporary | 5–10% |
| Neck stiffness and mild discomfortExpected during recovery | Common |
| Incision site discomfortTemporary | Common |
Persistent Complications (rare but possible)
| Complication | Rate |
|---|---|
| Persistent dysphagiaRequiring dietary modification or intervention | <1% |
| Implant subsidenceLeading to loss of disc height; rarely symptomatic | 1–5% |
| Implant malposition requiring revisionRare | <2% |
| Neurological deficit from operative complicationExceptionally rare | <1% |
| InfectionManaged with antibiotics or surgical washout | <1% |
Long-Term Considerations
Why Advanced ArthroplastyMatters
Advanced spinal arthroplasty—multilevel, hybrid, and complex scenarios—represents the frontier of motion-preserving spine surgery. By extending arthroplasty beyond single-level disease to carefully selected multilevel and complex patients, surgeons can achieve outcomes that were previously impossible.
Prevent Adjacent-Segment Disease Cascade
Motion preservation at multiple levels reduces biomechanical load on remaining mobile segments, potentially preventing future disease.
Improve Long-Term Outcomes
Patients maintain motion and function decades into the future; fusion cohorts show progressive adjacent-segment disease requiring escalating interventions.
Serve Younger Patients Optimally
Rather than condemning 45-year-olds to progressive three-level fusion, advanced arthroplasty preserves spinal motion and function across remaining lifespan.
Solve Complex Problems Creatively
Hybrid surgery, arthroplasty adjacent to prior fusion, and other creative approaches address clinical scenarios traditional surgery couldn't adequately handle.
Achieve Superior Long-Term Satisfaction
Patients undergoing appropriate advanced arthroplasty demonstrate 85–90% long-term satisfaction compared to 70–75% satisfaction with fusion cohorts.
Advanced arthroplasty is not appropriate for all patients with multilevel disease. Careful patient selection, detailed anatomical assessment, realistic expectations, and experienced surgeon expertise remain essential.
But for appropriately selected patients, advanced arthroplasty offers outcomes and long-term benefits superior to traditional multilevel fusion approaches.
Understanding these advanced techniques requires consultation with a specialist experienced in motion-preserving spinal surgery. The right approach depends on your individual anatomy, symptoms, and goals.