
Adjacent Segment Disease
Adjacent segment disease represents a complex pathophysiological process where spinal segments adjacent to a fused level undergo accelerated degeneration. Understanding this is essential for informed surgical decision-making and long-term spinal health.
Annual Incidence
2-5%
Cumulative symptomatic risk increases over time following spinal fusion.
10-Year Symptomatic Rate
10-20%
Percentage of fusion patients who develop clinical symptoms causally related to ASD.
Risk Reduction
50-60%
Significant decrease in ASD risk with motion-preserving disc replacement.
Defining the Pathological Spectrum
Adjacent segment disease encompasses degenerative changes that occur in spinal segments immediately adjacent to (superior or inferior to) a previously treated spinal level. Precise terminology is essential, as healthcare providers distinguish several related but distinct phenomena.
Adjacent segment pathology (ASP) serves as an umbrella term encompassing both radiographic degeneration and clinical disease, used interchangeably with adjacent segment disease.
Natural History & Timeline
Adjacent segment degeneration follows a generally predictable timeline following spinal fusion, with risk accumulating year-by-year across the patient's remaining lifetime.
Biomechanical Shift
Immediate biomechanical alterations occur. Early-onset ASD can be detected radiographically. Symptomatic disease is uncommon but possible in high-risk patients.
Progressive Degeneration
Degenerative changes become evident on sequential imaging. Approximately 20% of patients develop early-onset symptomatic ASD within this window.
Clinical Manifestation
Cumulative ASD rates reach 25–40% radiographically and 10–20% symptomatically. Reoperation rates begin to increase significantly.
Lifelong Surveillance
Continued progressive degeneration. At 15-year follow-up, cumulative symptomatic ASD rates can reach 30–40%, spanning the patient's remaining lifetime.
Annual Incidence Pattern
Most studies document annual ASD symptomatic incidence rates of 2–5% per year in the first decade, with rates remaining relatively constant or increasing in years 10–15, suggesting ongoing degenerative processes throughout follow-up.
Biomechanical Alterations Post-Fusion
The primary driver of ASD is the profound alteration in spinal mechanics that occurs when a segment is permanently immobilised. This creates a cascade of mechanical stress on adjacent levels.
Loss of Motion
Spinal fusion eliminates motion entirely at the treated level, fundamentally changing the preoperative biomechanical state.
Compensatory Hypermobility
Remaining unfused segments must increase their motion to compensate for the fused level, often increasing from 10-15° to 20-30°.
Altered Load Distribution
Fusion increases intradiscal pressures (20-40%) and shear loads (up to 115%) at adjacent segments.
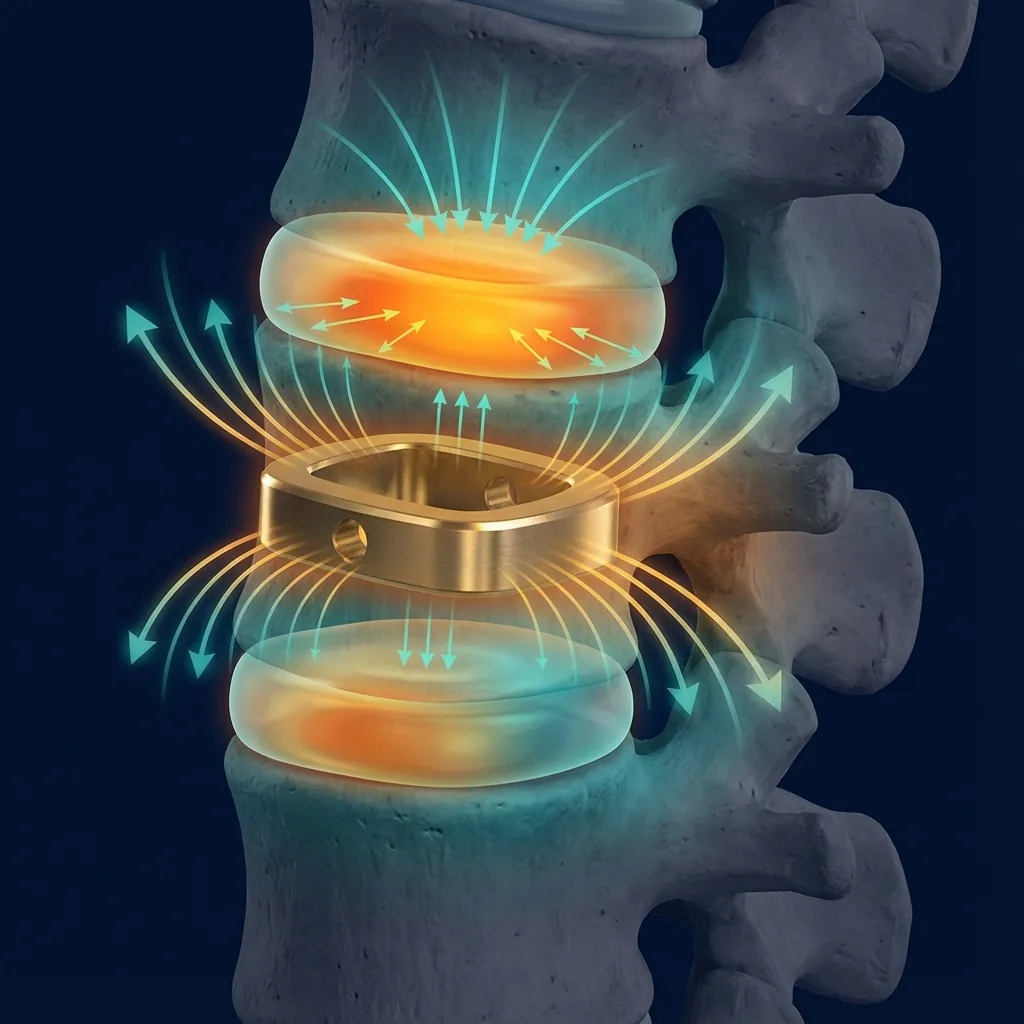
Load Concentration at Adjacent Levels
Visualisation of mechanical stress concentration following spinal fusion
Inflammatory Cascade
Increased production of IL-6, TNF-alpha, and prostaglandins at adjacent segments.
Matrix Breakdown
Accelerated degradation of proteoglycans and collagen fibres in the extracellular matrix.
Facet Joint Arthritis
Increased osteoclast activity and nerve invasion of subchondral bone in adjacent facets.
Iatrogenic Tissue Damage as a Catalyst
Extensive posterior approaches often require division of paraspinal muscles and posterior ligaments. This structural disruption impairs normal stabilisation and forces the unfused segments to bear the brunt of mechanical loads.
Removal of supraspinous and interspinous ligaments eliminates tension-band stability
Facet joint capsule disruption removes proprioceptive feedback
Paraspinal muscle atrophy impairs segmental stabilisation
Longitudinal Incidence Patterns
Incidence rates for adjacent segment disease vary significantly depending on the clinical endpoint, surgical region, and duration of follow-up.
Symptomatic ASDis
Radiographic degeneration accompanied by clinical symptoms (neck pain, arm pain, leg pain, or myelopathic symptoms) causally related to adjacent-segment degeneration.
Note: The wide range in reported incidence reflects differences in patient populations, imaging protocols, and definitions of ASD terminology. Not all radiographic degeneration progresses to symptomatic disease.
Multilevel Fusion Impact
Multilevel fusion constructs carry substantially higher ASD risk due to increased biomechanical burden on remaining mobile segments.
"The proximal (superior-most) adjacent segment bears the primary compensatory burden in long constructs."

Risk Velocity
Symptomatic ASD incidence remains relatively constant at approximately 2–5% per year, meaning cumulative risk builds reliably over decades.
Clinical Risk Architectures
Adjacent segment disease is multifactorial, occurring at the intersection of patient biology, surgical strategy, and intricate spinal anatomy. Understanding these risk factors enables prognostication and guides preventive strategies.
Patient-Specific Context
Age < 50 Years
Higher reoperation rates due to life expectancy and activity.
Pre-existing Degeneration
Radiographic changes pre-op dramatically increase risk.
Sagittal Imbalance
Positive sagittal balance increases loading on adjacent segments.
Obesity
Increases mechanical load and systemic inflammatory state.
Bone Marrow Oedema
Preoperative bone marrow oedema at adjacent vertebra dramatically increases risk (OR 16.8; 57% early-onset ASD within 2 years).
Surgical & Technical Variables
Length of Fusion
Multilevel constructs create exponentially greater stress.
Posterior Disruption
Muscle and ligament damage impairs normal stabilisation.
Excessive Distraction
Disc space widening >4mm creates biomechanical imbalance.
Instrumentation Type
Rigid pedicle screw systems carry standard high-risk baseline.
Pre-existing Conditions Amplify Risk
Pre-existing severe facet arthropathy (Grade 3–4) or severely degenerated discs at adjacent segments significantly increase the risk profile. Hypermobile segments are particularly susceptible to accelerated degeneration when the neighbouring level becomes rigid following fusion surgery.
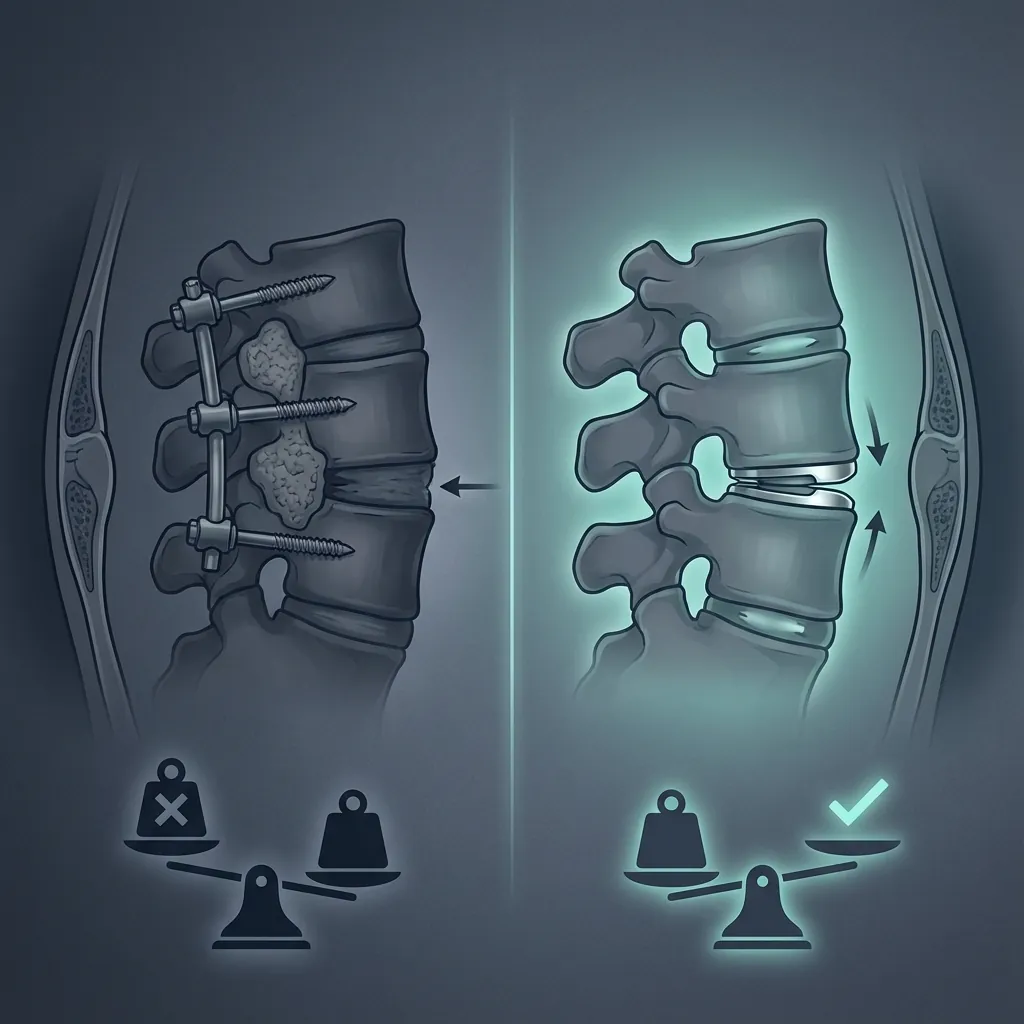
Motion Preservation vs Traditional Fusion
Extensive clinical meta-analyses demonstrate that motion-preserving procedures significantly reduce the incidence of adjacent segment degeneration and disease compared to traditional spinal fusion.
Radiographic Degeneration (7yrs)
Symptomatic ASD (7yrs)
Reoperation for ASD
The Protective Mechanism of Motion Preservation
Kinematic Maintenance
Motion is maintained at the index level, preventing the compensatory hypermobility forced upon adjacent segments in fusion constructs.
Physiological Loading
Load distribution remains distributed across the spinal column rather than concentrating at rigid interfaces.
Pressure Regulation
Intradiscal pressures at adjacent-segment discs remain substantially lower post-arthroplasty than post-fusion.
"Cervical disc replacement reduces reoperation for ASD by approximately 47–50% at 7-year follow-up when compared directly with ACDF."
Prevention Strategies& Long-term Management
Proactive prevention is the most effective approach to adjacent segment disease. By optimising surgical strategy, preserving motion where appropriate, and implementing comprehensive rehabilitation protocols, we can fundamentally alter the long-term prognosis.

Preoperative Optimisation
- Smoking cessation and weight management
- Bone mineral density optimisation
- Careful assessment of adjacent segments
- Restoring sagittal alignment preoperatively
Surgical Strategy
- Select tissue-sparing minimally invasive techniques
- Limit fusion extent to essential levels only
- Preserve posterior ligaments and facet joints
- Optimal disc space distraction (avoid >4mm)
Motion Preservation
- Disc arthroplasty for appropriate candidates
- Hybrid procedures for multilevel disease
- Maintaining physiological spinal kinematics
- 50-60% reduction in long-term ASD risk
Conservative Management
60–70% Success Rate"Most patients with symptomatic ASD initially benefit from systematic conservative treatment, aiming to avoid further surgical intervention where possible."
Anti-inflammatory medications (NSAIDs)
Stepwise targeted physiotherapy
Activity and ergonomic optimisation
Epidural or facet joint injections
Surgical Intervention
Patients failing conservative treatment after 6–12 weeks may be evaluated for surgical options ranging from decompressions to fusion extensions or motion-preserving arthroplasty at the adjacent level.
Patient Counselling Points
Risk of radiographic adjacent-segment degeneration increases with follow-up duration (approximately 25–40% by 10 years with fusion)
Risk of symptomatic ASD requiring treatment is lower (approximately 10–20% at 10 years with fusion)
Reoperation risk with fusion is approximately 5–15% at 10-year follow-up depending on fusion extent and technique
Motion-preserving approaches (disc replacement) reduce these risks by approximately 50%
Younger patients face higher long-term risk due to longer life expectancy
Careful surgical planning (minimising fusion extent, optimising technique) can reduce ASD risk
Cervical ASD Characteristics
ASD more often presents as recurrent cervical radiculopathy or myelopathy
Superior adjacent segment more commonly affected than inferior
Cervical arthroplasty shows greater ASD prevention benefit compared to lumbar
Three-level ACDF carries very high ASD risk (40% symptomatic at 10 years)
Lumbar ASD Characteristics
ASD more often presents as recurrent back pain or leg pain
Proximal (cranial) adjacent segment more commonly symptomatic than distal
Both disc and facet pathology may contribute to symptoms
Extended fusion constructs at the lumbosacral junction carry particularly high ASD risk
Early-Onset ASD (within 2 years)
Associated with specific perioperative risk factors (excessive distraction, bone marrow oedema)
May reflect accelerated degeneration in already-compromised segments
Patients with bone marrow oedema at adjacent level preoperatively have 57% early-onset ASD rate
Late-Onset ASD (>5 years)
Represents natural progression of degeneration accelerated by biomechanical alterations
Longer follow-up reveals continued progressive ASD development
Annual incidence rates remain constant through 15-year follow-up
Single-Level Disease
Motion-preserving approaches (disc replacement) significantly reduce long-term ASD risk. For appropriate candidates (good bone quality, preserved disc height, minimal facet disease), arthroplasty is preferred over fusion.
Two-Level Disease
ASD risk increases substantially. Hybrid approaches (replacement at one level, fusion at another) offer compromise balancing motion preservation with stabilisation. All-arthroplasty approaches appropriate for select candidates.
Multilevel Disease
Three-level fusion carries very high long-term ASD risk. Careful patient selection and conservative therapy optimisation essential. Hybrid approaches increasingly considered. Limited multilevel arthroplasty (two-level, rarely three-level) increasingly performed with good outcomes.
Patient-Specific Factors
Younger patients with longer life expectancy benefit more from motion-preserving approaches
Patients with minimal adjacent-segment degeneration preoperatively are better fusion candidates if indicated
Patients with preoperative bone marrow oedema at adjacent segments should strongly consider motion preservation
Final Synthesis: ASD & Clinical Decision-Making
Adjacent segment disease represents a fundamental challenge in spinal surgery. Understanding its pathophysiology should directly influence the choice to preserve motion, limit fusion extent, and employ tissue-sparing techniques.
ASD is common and progressively increases over months to years.
Biomechanical alteration is the primary mechanism of accelerated degeneration.
Prevention through careful planning is more effective than late-stage treatment.
Motion preservation can reduce ASD risk by 50–60% compared to fusion.
Fusion extent matters—single-level carries lower risk than multilevel.
Surgical technique, including minimally invasive approaches, optimises outcomes.
Remember
"Adjacent segment disease represents an inevitable consequence of spinal fusion—increased loads at adjacent unfused segments accelerate their natural degeneration."
"However, this outcome is not immutable. Careful surgical planning, patient selection, technique optimisation, and strategic use of motion-preserving approaches substantially reduce ASD development and the need for future operations."
Understanding adjacent segment disease should guide decisions about surgical approach, implant selection, and extent of intervention, with the goal of optimising both immediate pain relief and long-term spinal health across the patient's remaining lifetime.