Biomechanics Of Spinal Arthroplasty
The biomechanical science of spinal arthroplasty encompasses principles of mechanical engineering, materials science, and physiology. Modern disc replacements employ sophisticated design concepts to replicate the complex, multi-axial motion patterns of the natural spine whilst withstanding decades of cyclic loading.
Motion Freedom
Multi-Axial Movement
6 Degrees
Complete spinal motion through three translational and three rotational components enabling natural, unconstrained movement patterns.
Engineering Durability
Proven Performance
40+ Years
Modern implants withstand 40+ million loading cycles, approximating decades of physiological motion through rigorous materials science testing.
Lower ASD Risk
Adjacent Segment Protection
40-50%
Motion preservation reduces adjacent segment disease rates by 40-50% compared to fusion through physiological load distribution.
The Spine as a Dynamic SystemIntegrated Biomechanical Architecture
The human spine functions as an integrated biomechanical system comprising 24 mobile vertebrae, connected by intervertebral discs, facet joints, ligaments, and surrounding musculature. This complex architecture enables the spine to perform multiple simultaneous functions whilst maintaining structural integrity under demanding mechanical conditions.
Primary Biomechanical Functions

Understanding These Principles
Understanding biomechanical principles helps explain why different implant designs exist, how they compare to fusion approaches, and why appropriate patient selection is crucial for optimal outcomes.
Six Degrees of FreedomComplete Motion Characterisation
Spinal motion occurs through six degrees of freedom that define the complete range of movement possibilities at each vertebral level. This sophisticated kinematic framework encompasses both translational and rotational movements across three-dimensional space.
Three Translational Components
Three Rotational Components

Mechanical Coupling
Research demonstrates that these six degrees of freedom are mechanically coupled, meaning that loading in one direction affects the mechanics of all other movement planes. This coupling creates the complex, coordinated motion patterns that characterise normal spinal function and distinguish healthy movement from pathological conditions.
Load Distribution in Healthy Spinal MotionFoundation for Understanding Artificial Discs
Understanding normal load distribution patterns provides the foundation for appreciating how artificial discs must function to restore healthy biomechanics. The spine experiences complex loading patterns that vary dramatically with posture, activity, and external forces.
Physiological Load Patterns
The Role of Facet Joints
Facet joints play a crucial complementary role to intervertebral discs in spinal load distribution and motion control. Understanding this integrated function becomes essential when designing artificial disc replacements that must work harmoniously with existing anatomical structures.
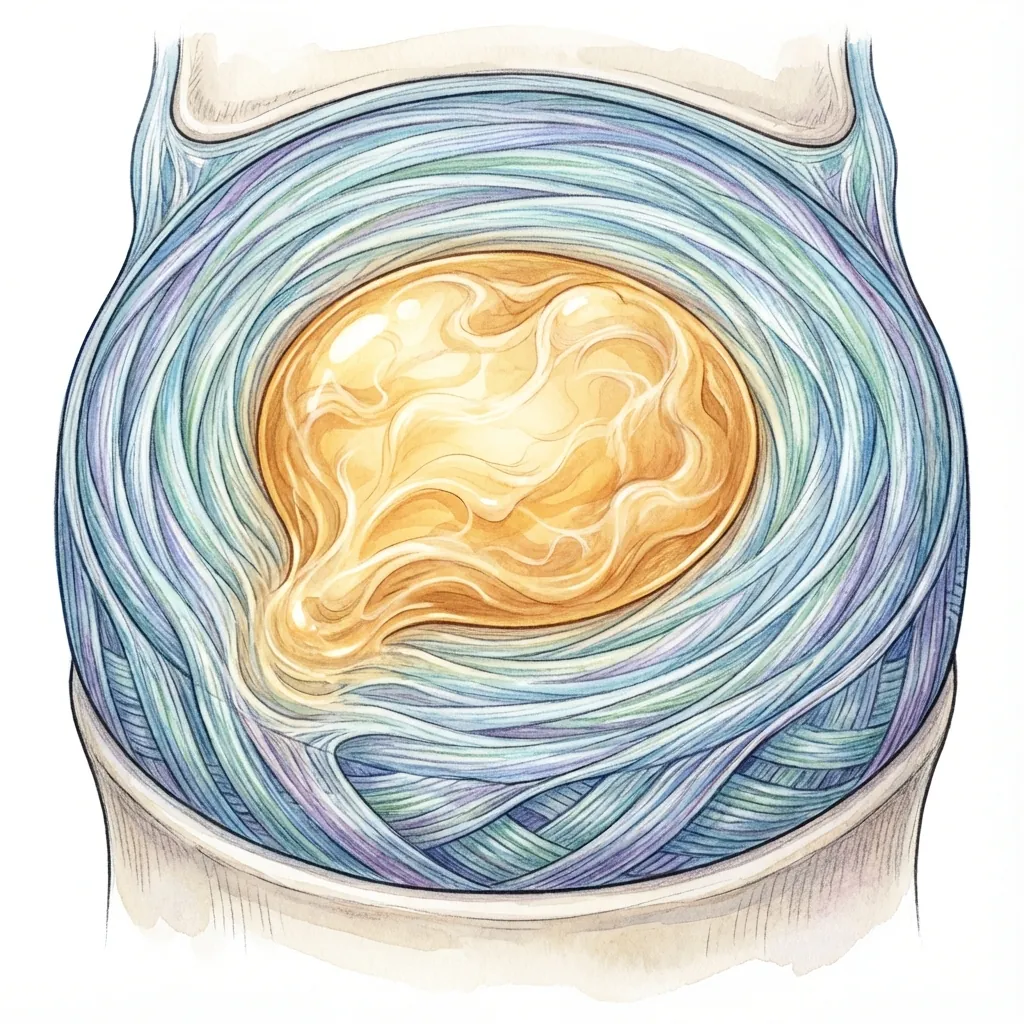
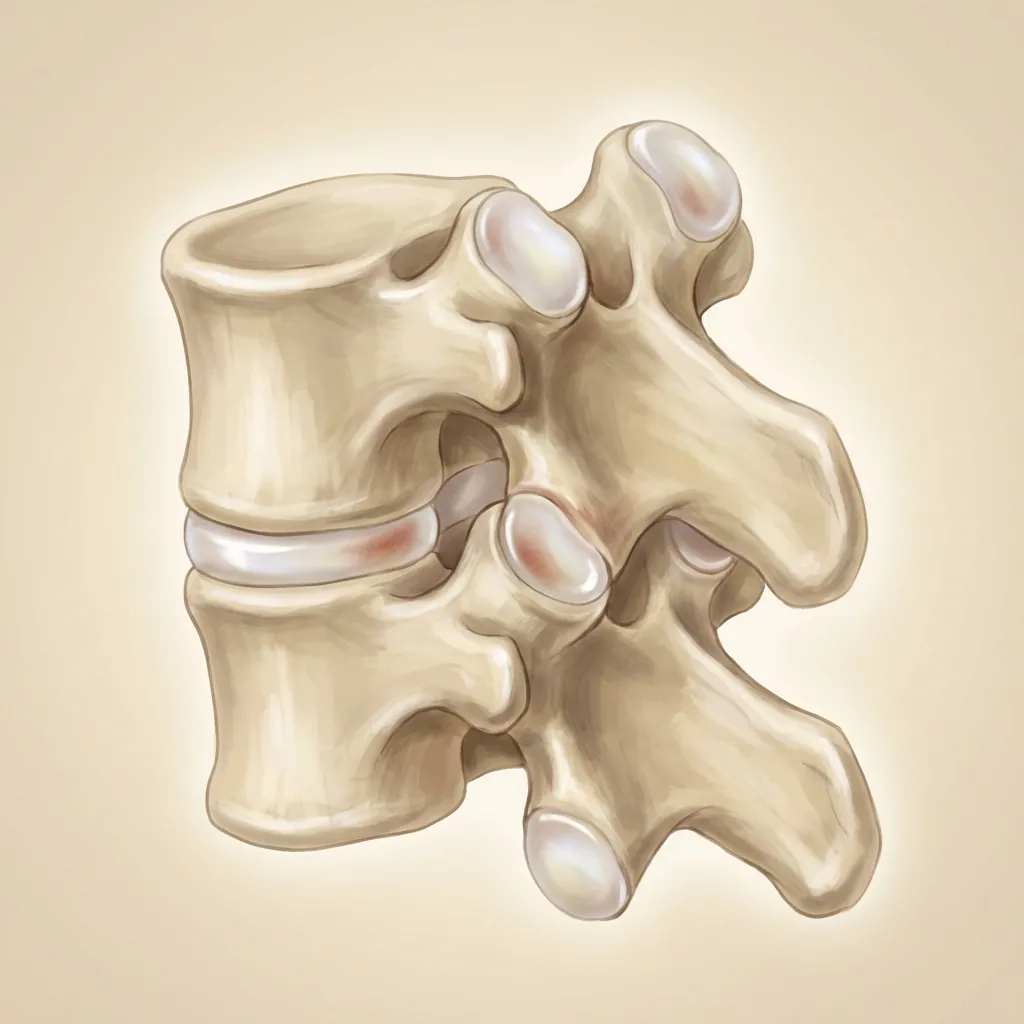
The Natural Spinal DiscEngineering Masterpiece
Before understanding artificial discs, appreciating the remarkable engineering of the natural human spinal disc is essential. The intervertebral disc consists of three primary components working in sophisticated harmony.
Structural Anatomy
Biomechanical Properties
Load Distribution
Distributes compressive loads across large surface area, preventing focal stress concentration. Under 1,000 N load (~100 kg), intradiscal pressure rises proportionally—roughly 0.5–1.0 MPa.
Variable Centre of Rotation
The natural disc does not have a fixed pivot point. During flexion it moves posteriorly; during extension, anteriorly. This allows smooth, non-constrained motion.
Viscoelastic Behaviour
Stiffness increases with loading rate and amount. Under light loads, the disc is relatively compliant; under heavy loads, it becomes stiffer—analogous to an automobile shock absorber.
Shock Absorption
The nucleus pulposus acts as a hydraulic shock absorber. Impact loads are converted into radial pressure that deforms the annulus, distributing force gradually.
Motion Patterns Per Segment
| Motion Type | Cervical | Lumbar |
|---|---|---|
| Flexion-Extension | 6–12° | 10–15° |
| Lateral Bending | 4–8° | 4–8° |
| Axial Rotation | 3–6° | 1–3° |
| A-P Translation | <2 mm | <2 mm |
Load-Bearing Capacity
The disc typically resists compression to approximately 10,000–20,000 N before catastrophic failure—a capacity rarely approached in normal human activity.
Biomechanical ConsequencesOf Disc Degeneration and Fusion
Understanding what goes wrong with spinal degeneration and how fusion alters biomechanics provides essential context for appreciating why motion-preserving approaches exist.
Primary Level (Degenerate Segment)
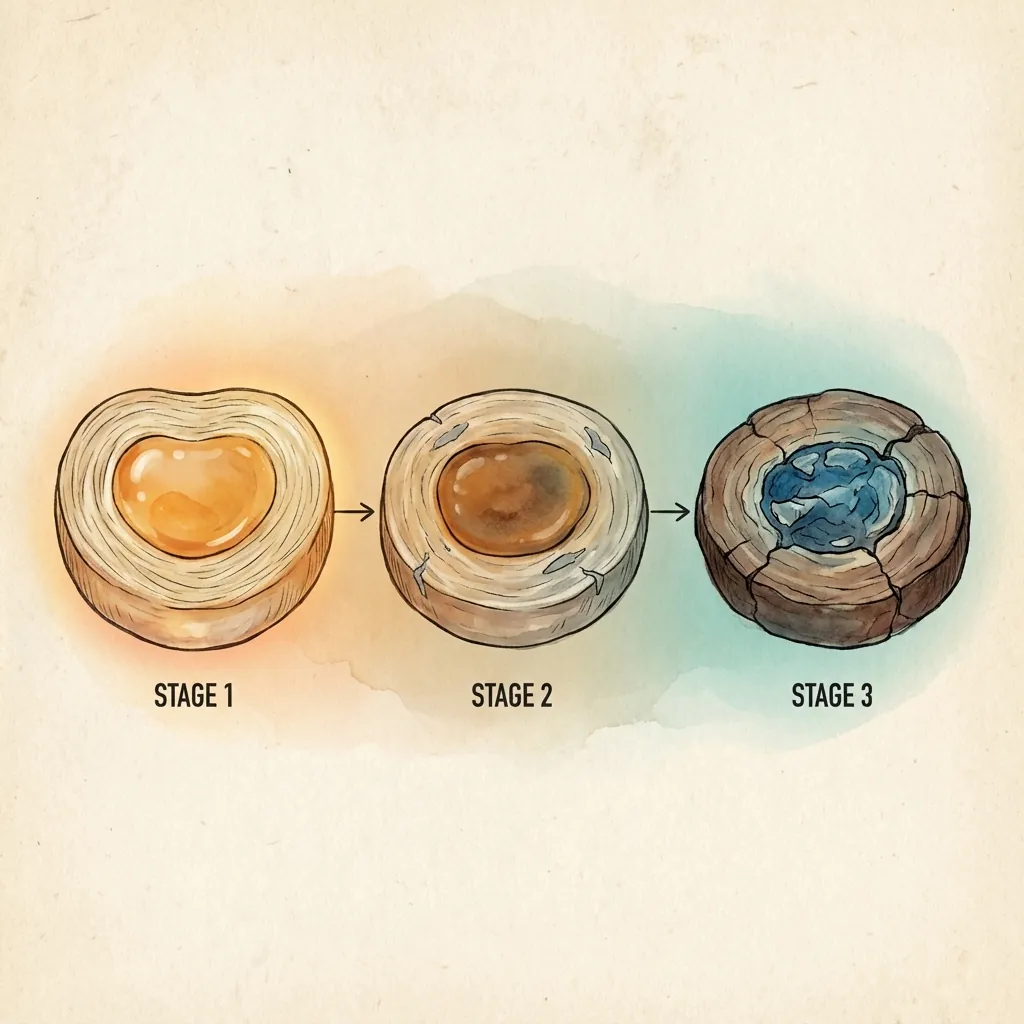
When a spinal disc degenerates, progressive biomechanical changes cascade through multiple spinal segments:
Nucleus loses hydration, becoming desiccated
Reduced shock absorption
Intradiscal pressure decreases
Altered load distribution
Disc height diminishes (typically 20–50% loss)
Nerve compression risk
Annulus develops fissures and tears
Structural weakness
Endplate cartilage degenerates
Nutrient pathway compromise
The segment becomes mechanically compromised
Motion segment dysfunction
Adjacent-Level Biomechanical Compensation
When one segment degenerates, adjacent unfused segments must compensate biomechanically:
Increased Range of Motion
Adjacent segments move excessively to maintain global spinal mobility.
Increased Intradiscal Pressure
Adjacent-segment discs experience elevated pressures as they absorb loads previously distributed across the degenerate level.
Altered Movement Patterns
Compensatory hypermobility creates abnormal kinematics not designed for sustained loading.
Increased Facet Loading
Adjacent facet joints experience increased force transmission beyond physiological norms.
Accelerated Degeneration
The excessive loading and abnormal motion patterns drive degenerative changes in adjacent discs and facet joints.
This biomechanical cascade explains why isolated degenerative disease often progresses to multilevel disease—mechanical compensation creates a self-perpetuating degenerative process.
Principles of Artificial Disc DesignSophisticated Engineering for Complex Biomechanics
Artificial disc implants represent sophisticated engineering solutions to a complex biomechanical problem: provide immediate stability, preserve motion, load-share (not rigidly fix), and maintain physiological loading patterns whilst withstanding decades of cyclic loading.
Fundamental Design Goals
All modern spinal disc replacements aim to achieve:
Design Philosophy Differences
Disc replacements fall into three primary design categories, each with different biomechanical philosophies:
First-Generation Articulating (Ball-and-Socket)
These implants feature a ball-shaped core articulating in a socket, mimicking a synovial joint. Examples include ProDisc and Prestige LP implants.

Advantages
- Well-understood, proven design concepts (adapted from hip arthroplasty)
- Long clinical track record with 15–20+ year follow-up data
- Reliable motion restoration
- Satisfactory outcomes in clinical practice
Biomechanical Considerations
- Fixed centre of rotation—does not mimic natural disc's variable centre
- Motion patterns are more constrained than the natural disc
- May permit excessive motion at facet joints
- Polyethylene wear possible over extended follow-up
- Intradiscal pressure at adjacent segments remains elevated compared to natural disc
Cervical Spine BiomechanicsAnd Motion Preservation
The cervical spine presents distinct biomechanical challenges that influence artificial disc design requirements and clinical outcomes.
Unique Cervical Biomechanical Requirements
Cervical Disc Replacement Biomechanics
Cervical artificial discs must address the specific biomechanical requirements of the neck whilst providing long-term durability and safety.
Centre of Rotation Considerations
The position of the centre of rotation critically influences cervical biomechanics. Devices with inappropriately positioned rotation centres can create abnormal facet joint loading and alter natural motion patterns, potentially leading to accelerated wear or clinical symptoms.
Motion Coupling Preservation
Successful cervical disc designs must maintain the natural coupling between different motion planes that characterises normal neck movement. This requires sophisticated engineering that accommodates complex three-dimensional motion patterns.
Facet Joint Protection
Cervical artificial discs must work in harmony with the facet joints to provide appropriate motion guidance and load distribution. Designs that create excessive facet loading may contribute to accelerated degeneration and clinical problems.
Clinical Biomechanical Outcomes
Clinical studies demonstrate the biomechanical success of cervical artificial disc replacement in maintaining natural motion patterns and protecting adjacent segments.
Motion Maintenance
Long-term studies show that cervical artificial discs maintain physiological ranges of motion throughout extended follow-up periods. This preserved mobility contributes to improved patient satisfaction and functional outcomes compared to fusion approaches.
Adjacent Level Protection
The protective effect on adjacent cervical levels is particularly pronounced, with studies showing more than 50% reduction in adjacent segment disease compared to fusion surgery. This biomechanical advantage translates into significant clinical benefits for patients.
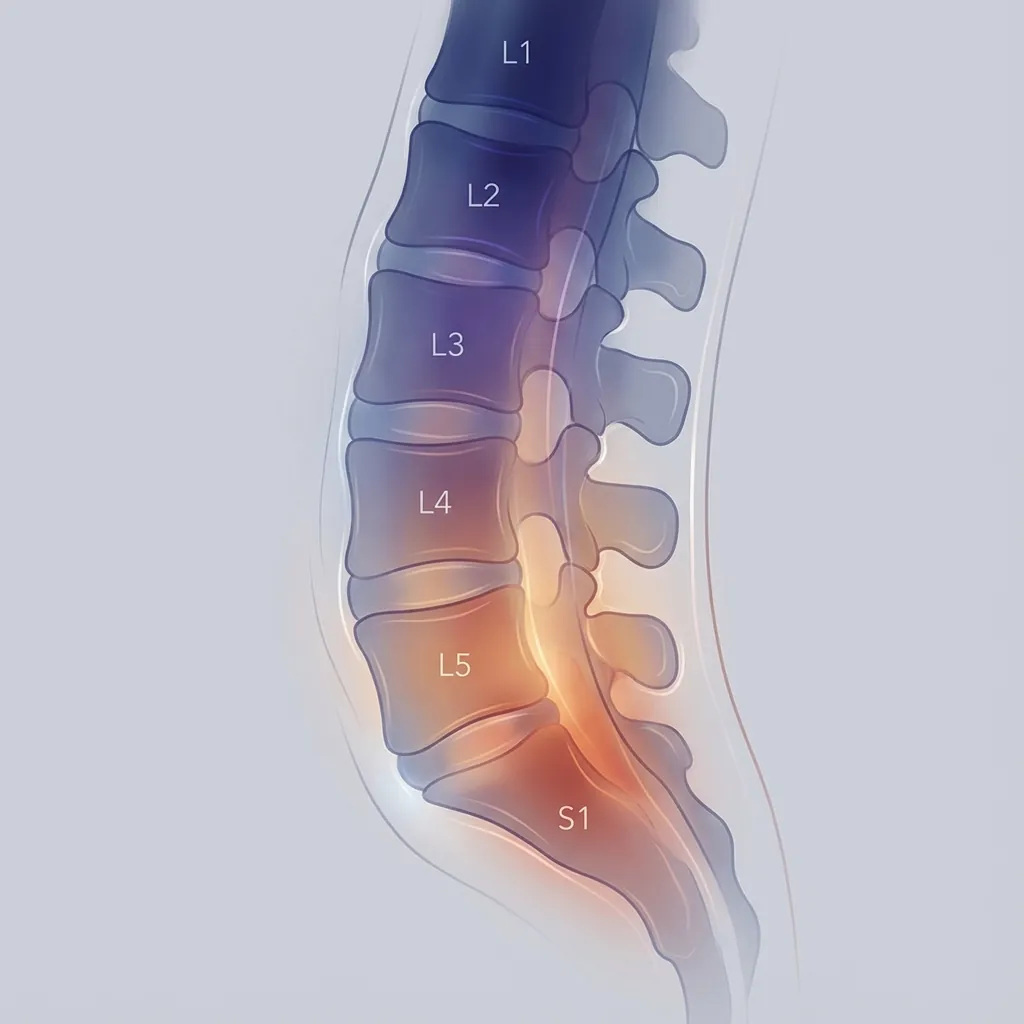
Lumbar Spine BiomechanicsAnd Artificial Disc Function
The lumbar spine experiences the highest loads in the spinal column whilst requiring significant mobility for activities of daily living. These demanding requirements create unique challenges for artificial disc systems.
Lumbar Biomechanical Challenges
Anterior Approach Biomechanical Considerations
The anterior surgical approach used for lumbar disc replacement provides important biomechanical advantages whilst creating specific technical requirements.
Complete Disc Removal
The anterior approach enables complete removal of degenerative disc tissue, ensuring optimal preparation of the disc space for artificial disc implantation. This complete discectomy is essential for proper load distribution and implant stability.
Large Footprint Capability
Anterior access allows implantation of large-footprint devices that maximise load distribution across the vertebral endplates. This biomechanical advantage reduces subsidence risk and ensures appropriate load transmission characteristics.
Anatomical Restoration
The anterior approach facilitates restoration of normal disc height and spinal alignment, crucial factors for maintaining physiological biomechanics and preventing accelerated degeneration of surrounding structures.
Biomechanical Advantage Summary
Ball-and-Socket Implant BiomechanicsEstablished Clinical Performance
Ball-and-socket implants represent the most clinically established design category, with the largest body of long-term outcome data spanning 15–20+ years of follow-up.
Mechanical Structure:
A 2021 finite element analysis comparing ball-and-socket designs (Prestige LP and CSDP prosthesis) to intact spine found:
| Parameter | Flexion-Extension | Lateral Bending | Axial Rotation |
|---|---|---|---|
| Intact Spine | 29.6° | Comparable | Comparable |
| CSDP Prosthesis | 28.9° (2.4% ↓) | Comparable | Comparable |
| Prestige LP | 31.8° (7.6% ↑) | Comparable | Comparable |
Adjacent-segment motion patterns remained physiological with compensatory hypermobility less pronounced than with fusion.
Ball-and-socket designs typically have a semi-fixed or fixed centre of rotation located at the articulation point. This differs from the natural disc:
Clinical significance: This fixed-centre characteristic means ball-and-socket implants create more constrained motion patterns than natural discs. The motion is smooth and satisfactory but somewhat artificial compared to natural spinal mechanics.
A 2019 biomechanical study using cadaveric cervical specimens tested facet joint contact forces with Prestige LP implants:
| Motion Type | Force Range | Finding |
|---|---|---|
| Extension | 15–20 N | Maintained near-normal |
| Lateral Bending | 10–15 N | Similar to intact |
| Axial Rotation | 8–12 N | Within physiological range |
Comparison to fusion: Fusion significantly reduced facet joint contact forces at the operative level (6.9 N vs 13.4 N in bending), but created compensatory load increases at adjacent facet joints.
A 2022 finite element study comparing ACDF to artificial disc arthroplasty (Bryan and Prestige LP) found:
| Treatment | Nucleus Stress | Annulus Stress | IDP Change |
|---|---|---|---|
| Preoperative Intact | Baseline | Baseline | 0% |
| ACDF Fusion | Elevated 20–30% | Elevated 15–25% | Increased |
| Bryan Arthroplasty | Baseline to slightly elevated | Baseline to slightly elevated | Maintained |
| Prestige LP | Baseline to slightly elevated | Baseline to slightly elevated | Maintained |
Key finding: Arthroplasty maintained intradiscal pressures at adjacent segments close to preoperative levels, whilst fusion significantly elevated them.
One potential concern with ball-and-socket designs involving polyethylene is wear over extended follow-up.
Clinical observations: Modern ProDisc implants show minimal wear after 40 million cycles (approximately 15–20 years of physiological motion). Current generation implants demonstrate excellent long-term durability.

Viscoelastic Implant BiomechanicsNon-Articulating Design Philosophy
Second-generation viscoelastic disc implants represent an emerging design philosophy attempting to more closely replicate the natural disc's complex mechanical behaviour through deformable elastomeric or composite cores.
Rather than articulating ball-and-socket joints, viscoelastic designs feature deformable elastomeric or composite cores that:
Natural disc analogy: The natural disc's nucleus compression and nucleus pulposus movement creates fluid redistribution. Viscoelastic designs attempt to replicate this hydro-mechanical behaviour through elastic material deformation.
2020 review of viscoelastic disc designs (LP-ESP, M6-L, and others):
Six Degrees of Freedom:
Comparison to Natural Disc:
- • Closely approximates natural disc's six degrees of freedom
- • More physiological motion patterns than ball-and-socket designs
- • Variable centre of rotation mimics natural biomechanics
A 2025 landmark biomechanical study published peer-reviewed comparisons of the AxioMed VTDR to native human lumbar discs:
Stiffness Comparisons Under Physiologic Loading:
| Parameter | AxioMed VTDR | Native Lumbar Disc | Match Quality |
|---|---|---|---|
| Axial Stiffness | 4,800–5,200 N/mm | 4,500–6,500 N/mm | Excellent overlap |
| Flexion-Extension | 150–180 Nm/deg | 140–200 Nm/deg | Excellent overlap |
| Axial Rotation | 0.79–0.83 Nm/deg | 2.0–9.6 Nm/deg | Good (provides mobility) |
| Compressive Shear | 0.49–0.59 kN/mm | 0.4–0.7 kN/mm | Excellent overlap |
Key findings:
- • Nonlinear load response: Stiffness increased with loading magnitude, replicating natural disc behaviour
- • Durability: No failures under static compression to 20,000 N
- • First viscoelastic design demonstrated to replicate lumbar disc stiffness more closely than prior designs
This represents a fundamental advancement in biomechanical alignment between artificial and natural discs.
Elastomer Attachment to Metal Endplates:
Viscoelastic implants must firmly attach the elastic core to rigid metal endplates. Two attachment strategies exist:
Overmolding (Direct Fixation)
Elastomeric material bonded directly to metal endplate.
Fiber-Reinforced Attachment (M6-L Design)
Ultrahigh-molecular weight polyethylene fibres wound around elastic core creating friction contact with metal endplates.
Movement Limiters (LP-ESP Design Example):
- • Central silicone nucleus surrounded by PCU annulus
- • Mechanical limiters control axial translation and compression
- • Asymmetrical design prevents kyphosis
- • Purpose: protect facet joints and prevent hypermobility
15-Year Experience with LP-ESP Viscoelastic Design:
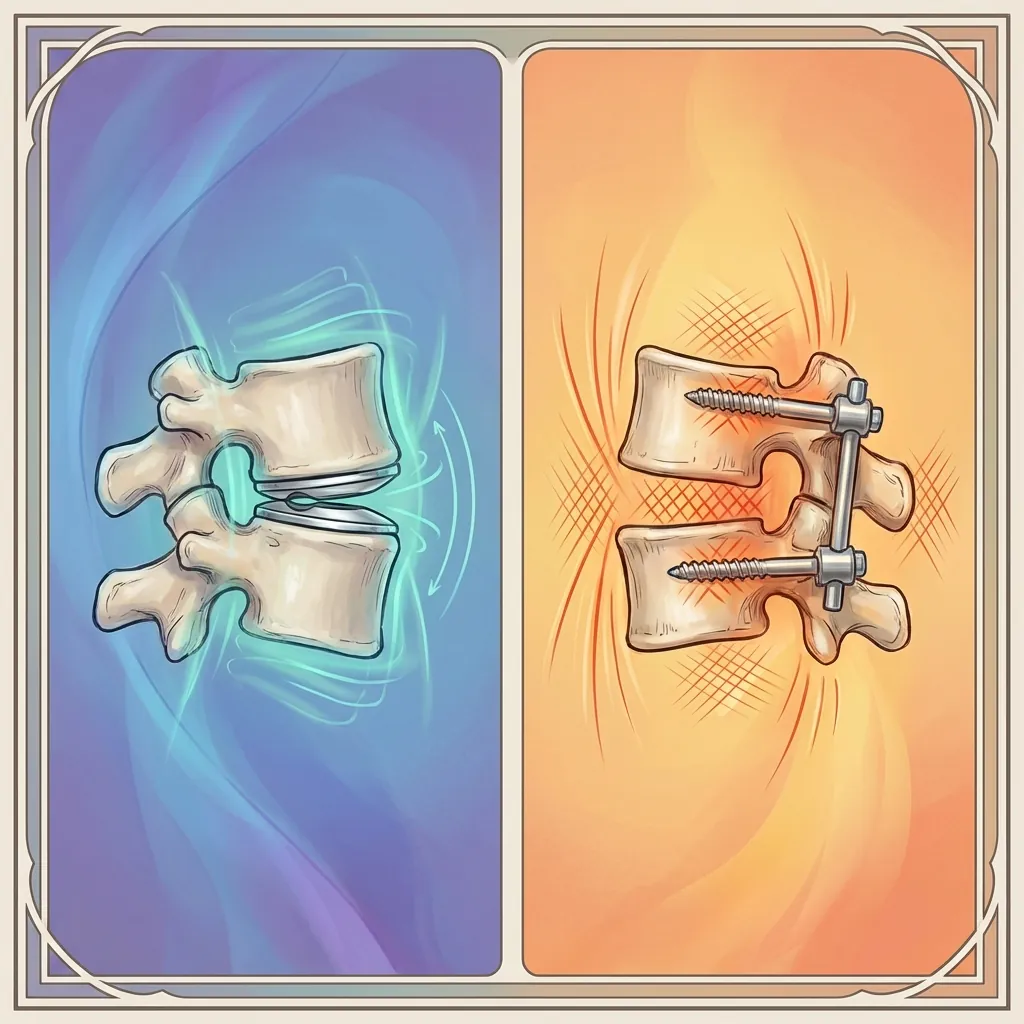
Comparative BiomechanicsArthroplasty vs Fusion vs Hybrid
Direct biomechanical comparisons reveal the fundamental differences between surgical approaches and their impact on spinal mechanics.
A 2022 finite element study directly compared cervical ACDF (fusion), Bryan disc arthroplasty, and Prestige LP arthroplasty at C5–C6.
Range of Motion at Operative Level
| Approach | Flex-Ext | Lateral | Axial |
|---|---|---|---|
| Intact Spine | 8–10° | 5–8° | 4–6° |
| ACDF Fusion | 0° (complete immobility) | 0° | 0° |
| Bryan Arthroplasty | 7.5–9° | 6.5–8° | 5–7° |
| Prestige LP | 8–10° | 6–7° | 5–6° |
Intradiscal Pressure at Adjacent Segments
| Parameter | Fusion | Arthroplasty |
|---|---|---|
| IDP Increase vs Preop | +250–550% | +10–50% |
| Absolute Pressure Elevation | Highest (0.5–1.2 MPa additional) | Minimal (0.05–0.25 MPa additional) |
| Annulus Fibrosus Stress | Elevated 15–25% | Baseline to slightly elevated |
| Facet Joint Force | Reduced at operative; elevated at adjacent | Maintained near physiological |
Interpretation
Fusion eliminates motion completely but dramatically elevates loading at adjacent segments. Arthroplasty preserves motion and maintains near-physiological loading at adjacent segments.
Intradiscal PressureThe Key Biomechanical Parameter
Intradiscal pressure (IDP) is arguably the most clinically significant biomechanical parameter, as it directly correlates with disc stress, degeneration risk, and long-term outcomes.
Normal Physiological Intradiscal Pressures
These pressures reflect the nucleus pulposus generating hydraulic pressure as it distributes compressive loads radially.
IDP Changes with Surgical Intervention
Impact of Fusion
above baseline (highest within 2–3 segments)
throughout follow-up
degenerative disc disease at adjacent levels
Impact of Arthroplasty
above baseline (minimal elevation)
at operative level
adjacent-segment disease rates
Clinical Correlation: IDP and Disease Progression
Studies examining patients with baseline bone marrow edema (BME) in adjacent-segment discs found:
increased risk of adjacent-segment disease with baseline bone marrow edema (BME) present
of patients with preoperative BME developed early-onset ASD (within 2 years)
Interpretation: Elevated IDP damages disc cells and accelerates degenerative changes, particularly in discs already showing signs of structural stress.
Facet Joint BiomechanicsAnd Loading Patterns
The facet joints (posterior spinal joints) transmit 15–40% of compressive loads and are critical load-bearing structures. Surgical intervention alters facet joint loading patterns with long-term consequences.
Intact Spine Facet Forces (Normal Reference)
Cervical spine biomechanical testing data:
Facet Joint Loads with Different Surgical Approaches
ACDF Fusion Impacts
Arthroplasty Impacts
Heterotopic Ossification and Facet Loading
Theory: Higher facet joint forces may stimulate reactive bone formation. Ball-and-socket designs, particularly Prestige LP, are associated with higher cervical facet forces than some articulating designs, potentially explaining observed heterotopic ossification patterns.
Clinical Data:
Biomechanical studies identify increased facet loading with Prestige LP, suggesting a possible mechanistic link to heterotopic ossification.
Shock AbsorptionAnd Energy Dissipation
One critical function of the natural disc is shock absorption—converting impact forces into distributed energy dissipation rather than stress concentration.
Natural Disc Shock Absorption Mechanism
The natural disc absorbs energy through four integrated mechanisms:
Nucleus Deformation
Hydraulic absorption distributes load radially across the disc structure.
Annulus Elastic Recoil
Collagen fibres deform and rebound, storing and releasing energy.
Fluid Redistribution
Water moves within the gel matrix, distributing forces over time.
Viscous Damping
Fluid movement creates internal friction and energy dissipation.
Result: Impact loads are converted into distributed pressure gradients rather than focal stress spikes.
Shock Absorption in Artificial Discs
Ball-and-Socket Designs
- Limited shock absorption capability
- Motion is relatively constrained and non-compliant
- Loads are more concentrated at articulation point
- Reduces shock-absorption effectiveness
Viscoelastic Designs
- Material deformation provides shock absorption
- Elastic core compresses and rebounds
- Fibre reinforcement in some designs provides damping
- Better approximates natural disc's energy dissipation
Clinical Significance
Improved shock absorption theoretically reduces:
- Impact-related microtrauma to endplates
- Stress concentration at adjacent segments
- Noise and vibration transmission through the spine
- Long-term degenerative changes
However, clinical evidence demonstrating superiority of viscoelastic designs over articulating designs in shock absorption is still emerging.
Sagittal AlignmentAnd Biomechanical Balance
Sagittal alignment—the balance between spinal curvature and pelvic orientation—profoundly influences biomechanical loading patterns and clinical outcomes.
The Importance of Sagittal Balance
Key sagittal parameters influence spinal biomechanics:
Pelvic Incidence (PI)
Fixed anatomical parameter determining pelvic requirements for sagittal balance.
Lumbar Lordosis (LL)
Crucial variable that should match pelvic incidence for optimal mechanics.
PI-LL Mismatch
Discrepancy between pelvic incidence and lordosis indicating sagittal imbalance.
Sagittal Vertical Axis (SVA)
Global measure of forward lean; elevated SVA correlates with poor outcomes.
Cervical Lordosis
Normal cervical lordosis is approximately:
How Surgical Approaches Affect Sagittal Parameters
Fusion Surgery's Impact
- Rigid fixation maintains operative-level sagittal parameters
- May or may not adequately restore lordosis depending on cage angle
- Long-segment fusions can alter global balance
- Fixed position cannot accommodate postural adjustments
Arthroplasty's Impact
- Implant height and angle can restore segmental lordosis
- Motion preservation allows postural adaptation
- Does not rigidly lock spinal alignment
- May accommodate physiological adjustments over time

Patient Selection Insight
Appropriate implant selection requires consideration of sagittal alignment needs, particularly for patients with existing sagittal imbalance.
Range of MotionAnd Quality of Motion
Beyond simply measuring degrees of motion, the quality and characteristics of that motion matter for long-term outcomes.
Quantitative ROM Assessment
Artificial discs maintain motion close to physiological norms:
| Level | Metric | Post-Arthroplasty | Normal |
|---|---|---|---|
| C5–C6 | Flexion-Extension ROM | 6–10° | 8–12° |
| C6–C7 | Flexion-Extension ROM | 5–8° | 6–10° |
| L4–L5 | Flexion-Extension ROM | 10–15° | 12–18° |
| L5–S1 | Flexion-Extension ROM | 8–12° | 10–15° |
Quality of Motion Parameters
Smoothness
Absence of catches, jerks, or erratic motion during movement arc.
Centre of Rotation Behaviour
How the instantaneous centre of rotation moves during motion (ideally variable, like natural disc).
Coupling Patterns
Coordination between primary and secondary motion planes (e.g., rotation coupled with lateral bending).
End-Range Characteristics
Behaviour at extremes of motion—soft stop vs. hard stop, resistance patterns.

Long-Term Motion Maintenance
Critical question: Does motion persist over decades?
ProDisc 10-year data
Maintained >80% of immediate postoperative ROM
Prestige LP long-term
Preserved in 85–90% of patients
Bryan 10-year data
Maintained in majority
Clinical Significance
Long-term data confirms that artificial disc motion is durable. Motion losses, when they occur, are typically associated with heterotopic ossification rather than implant failure.
Materials ScienceAnd Durability
Artificial discs must withstand millions of loading cycles over decades—a demanding materials science challenge that has driven significant engineering innovation.
Long-Term Durability Requirements
Implants must maintain function through approximately 1–2 million loading cycles per year:
Material Options
Cobalt-chrome or titanium endplates with UHMWPE (ultra-high molecular weight polyethylene) core.
Advantages
- Well-established track record from hip arthroplasty
- Excellent biocompatibility
- Good wear characteristics
- Low friction
Considerations
- Polyethylene wear over decades
- Potential for wear debris
- Height loss over time (minimal with current materials)
Titanium-ceramic composite or stainless steel on stainless steel articulation.
Advantages
- No polyethylene wear concerns
- Excellent durability
- Thin profile possible
- High strength
Considerations
- Metal ion release potential
- Requires careful manufacturing
- Higher cost
Polyurethane, silicone, or composite cores bonded to metal endplates.
Advantages
- Viscoelastic behaviour mimics natural disc
- Shock absorption capability
- Variable centre of rotation
- No articulating wear
Considerations
- Long-term material degradation unknown
- Attachment failure potential
- Limited long-term clinical data

Clinical Durability Evidence
ProDisc (UHMWPE)
Less than 0.8 mm height loss after 40 million cycles
Prestige LP (Metal)
No case of implant failure from wear in published studies
LP-ESP (Elastomeric)
No core delamination or material failure in clinical series
Materials Science Conclusion
Current generation artificial discs demonstrate excellent material durability throughout extended follow-up periods. Material failure as a revision indication remains rare.
Summary and Key TakeawaysBiomechanical Foundation for Decision-Making
Understanding spinal biomechanics provides the foundation for appreciating why motion-preserving approaches exist and how they differ from traditional fusion surgery.
Key Takeaways
Motion Preservation Matters
Preserving spinal motion reduces mechanical stress at adjacent segments, potentially lowering adjacent-segment disease rates by 40–50% compared to fusion.
Multiple Design Philosophies Exist
Ball-and-socket designs have the longest clinical track record; viscoelastic designs may offer more physiological motion characteristics. Both achieve excellent outcomes.
Evidence Supports Long-Term Durability
Modern artificial discs maintain motion and function throughout 15–20+ years of follow-up, with excellent material durability and low revision rates.
Patient Selection is Critical
Biomechanical benefits are maximised when implants are used in appropriately selected patients with preserved facet joints and suitable spinal alignment.
Fundamental Biomechanical Principles
The spine functions as an integrated biomechanical system requiring motion, stability, and load distribution
Six degrees of freedom characterise natural spinal motion—artificial discs aim to preserve this complexity
Intradiscal pressure and facet joint loading are key parameters influencing long-term outcomes
Fusion eliminates motion at the operative level but elevates stress at adjacent segments
Motion preservation approaches maintain more physiological loading patterns throughout the spine
Clinical Implications
Adjacent Segment Protection
Motion preservation significantly reduces the biomechanical drivers of adjacent-segment disease.
Long-Term Function
Maintained motion contributes to preserved quality of life and functional outcomes.
Durable Results
Current generation implants demonstrate excellent durability throughout extended follow-up.
For Patients
This biomechanical foundation helps explain why your surgeon may recommend artificial disc replacement in appropriate cases, and why the technology continues to evolve towards more physiological motion restoration.
The ultimate goal remains consistent: restoring pain-free function whilst preserving the spine's remarkable natural mechanics.
Understanding biomechanics empowers informed decision-making