Spinal Arthroplasty Case Studies Cervical & Lumbar
Realistic patient scenarios demonstrating clinical decision-making, surgical approaches, and long-term outcomes. These cases illustrate the spectrum of presentations, complexity of treatment selection, and actual results experienced in contemporary spinal arthroplasty practice.
Patient Scenarios
Cervical & Lumbar
8 Cases
Detailed case studies covering single-level radiculopathy, multi-level myelopathy, hybrid constructs, and complication management.
Patient Satisfaction
Long-Term Outcomes
85–95%
Evidence-based outcomes demonstrating excellent pain relief, functional restoration, and sustained motion preservation across all case categories.
Segmental Function
85–90% of Normal
Motion Preserved
Arthroplasty patients maintain near-normal spinal motion, reducing adjacent-segment disease risk compared to fusion surgery.
Understanding Spinal Arthroplasty
Rather than presenting idealised perfect outcomes, these cases demonstrate the spectrum of patient presentations, decision-making complexity, and actual results experienced in clinical practice. Each case illustrates the clinical decision-making process, surgical approaches, and long-term outcomes associated with cervical and lumbar spinal arthroplasty.

What These Cases Demonstrate
Cervical Arthroplasty
2 Detailed Cases- Case 1: Classic C6 radiculopathy — single-level
- Case 2: Two-level myelopathy — C4–C5 and C5–C6
Lumbar Arthroplasty
4 Detailed Cases- Case 3: L5–S1 radiculopathy with claudication
- Case 4: L4–L5 axial low back pain predominance
- Case 5: L5–S1 with Grade 1 anterolisthesis
- Case 6: Hybrid surgery — multilevel disease
Classic C6 Radiculopathy
Single-Level C5–C6 Disc Replacement
Margaret, 51
Retired accountant, Melbourne
6 Months
Progressive right-sided neck pain
62 min
Blood loss: 75 mL
95/100
Satisfaction score at 1 year
Patient Profile
Age / Gender
51 / Female
Occupation
Retired accountant
Location
Melbourne metropolitan area
Diagnosis
Right C6 Radiculopathy
Key Symptoms
Treatment Summary
This case exemplifies the ideal arthroplasty candidate and excellent outcome — clear single-level disease, failure of conservative care, appropriate patient selection, and technically successful procedure with excellent symptom relief.
Demographics
- Melbourne metropolitan area
- 30 years desk-based work requiring precise vision and fine motor coordination
- Private health insurance with moderate gap coverage
Comorbidities
- Mild hypertension (controlled)
- BMI 24 (healthy weight)
- Non-smoker
Margaret presented with a six-month history of progressive right-sided neck pain radiating into the right thumb and index finger. Pain intensity varied from 3/10 on good days to 8/10 on bad days, significantly affecting her quality of life.
Pain Characteristics
- • Sharp, burning quality radiating from neck base along lateral arm to thumb
- • Difficulty gripping utensils, writing, fine detail work
- • Avoided holding grandchildren for extended periods
Sleep Disturbance
- • Waking 2–3 times nightly due to pain
- • Numbness in hand causing night dysfunction
- • Gradual worsening over six months
- • Recent two weeks of significantly increased pain and weakness
Prior Conservative Care
Six weeks of physiotherapy with modest initial benefit (20% improvement), then plateau. One cervical epidural steroid injection providing three weeks symptom relief, then recurrence.
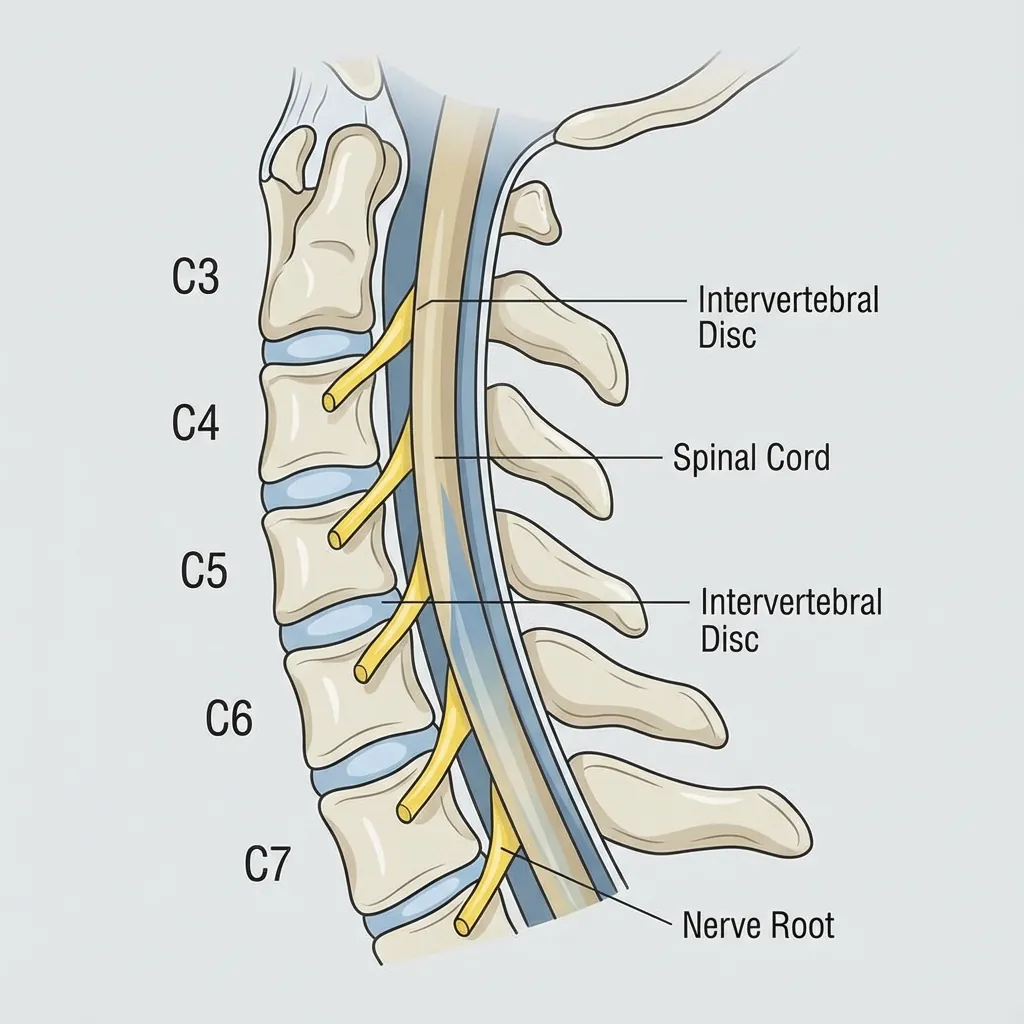
MRI Cervical Spine
- C5–C6: Moderate right-sided disc herniation compressing the right C6 nerve root in the neural foramen
- • Disc space height decreased compared to adjacent levels
- • Signal intensity in disc reduced (indicating dehydration/degeneration)
- • Spinal cord: Normal signal, no compression
- • C4–C5 and C6–C7: Mild degenerative changes, asymptomatic
CT Cervical Spine
- • Adequate vertebral body heights and endplate quality
- • Pedicle anatomy: Normal bilateral, suitable for instrumentation if future fusion required
- • Facet joints: Grade 1–2 osteoarthritis (mild)
- • Right C6 foramen narrowed by approximately 40% due to disc material and osteophyte
Dynamic X-rays (Flexion-Extension)
- • Segmental motion C5–C6: Approximately 8° (normal range 10–12°)
- • No excessive translation or instability
- • Cervical lordosis: Well-preserved
Physical Examination
- • Right triceps strength 4+/5 (mild weakness)
- • Diminished sensation in right C6 distribution
- • Right biceps reflex diminished
- • Spurling test: Positive on right
Diagnostic Impression
Right C6 radiculopathy secondary to C5–C6 disc herniation, single-level disease, excellent imaging-clinical correlation.
Margaret was assessed as an excellent candidate for cervical arthroplasty based on multiple factors.
Why Arthroplasty
- ✓ Single-level disease with clear imaging correlation
- ✓ Radicular pain pattern (not facet or multi-level)
- ✓ Adequate bone quality on imaging
- ✓ Mild facet joint involvement
- ✓ Preserved disc height
- ✓ Failure of conservative care
- ✓ Patient age and long life expectancy
Fusion vs Arthroplasty
Adjacent-segment disease risk:
• Fusion: 25–30% within 10 years
• Arthroplasty: 5–10% within 10 years
Motion preservation:
• Arthroplasty preserves 85–90% normal motion
Patient Decision Factors
Projected life expectancy into late 80s (decades of potential benefit), strongly valued maintaining spinal mobility and avoiding progression of adjacent segments. Comfortable with newer motion-preserving technology given evidence base.
Elected Treatment: Anterior cervical discectomy and insertion of cervical artificial disc (ACDA) at C5–C6 using ProDisc-C implant.
62 min
Operative Time
75 mL
Blood Loss
0
Complications
Three-Month Follow-Up Assessment
| Metric | Preoperative | 3 Months Post-op | Change |
|---|---|---|---|
| Neck Disability Index | 58/100 (severe) | 18/100 (minimal) | 69% improvement |
| Neck Pain (VAS) | 7/10 | 1/10 | 6-point improvement |
| Arm Pain (VAS) | 8/10 | 0/10 | Complete resolution |
| Grip Strength | 28 kg | 35 kg | Normalised |
| Return to Work | Off work | Full duty | Achieved by week 10 |
One-Year Follow-Up
- • Sustained symptom relief: Neck pain 0–1/10, radicular symptoms resolved
- • Full return to all prior activities (fine detail work, grandchild care, recreational activities)
- • Triceps strength 5/5 (normal); sensation fully normalised
- • Imaging: Stable implant, preserved segmental motion (7–8°, 85% of preoperative)
- • No complications; no adjacent-level symptoms
- • Patient stated surgery "completely restored my quality of life"
Clinical Significance
- Clear single-level disease matching clinical presentation
- Failure of conservative care establishing surgical necessity
- Appropriate patient selection with good bone quality and minimal facet disease
- Technically successful procedure with excellent symptom relief
- Motion preservation demonstrated on imaging
- No complications throughout follow-up
- Sustained improvement at one-year follow-up
- Patient very satisfied with outcome
Outcome Achieved
95/100 Satisfaction
Cervical Myelopathy
Hybrid Surgery: C5-C6 ADR + C6-C7 ACDF

Recovered
4 Weeks
0/10
Patient Profile
Age / Gender
45 / Male
Occupation
IT Systems Architect
Diagnosis
Cervical Myelopathy
Key Symptoms
Treatment Summary
This multi-level case demonstrates how hybrid constructs can effectively treat complex myelopathy while preserving motion.
A 45-year-old male presented with a 6-month history of progressive clumsiness in his hands and difficulty with balance while walking. He reported dropping objects frequently and feeling "unsteady" on his feet, particularly in low light. Neck pain was present but was a secondary complaint compared to the neurological symptoms.
Neurological Examination
- Positive Hoffman's sign bilaterally (indicating spinal cord irritation)
- Hyperreflexia in upper and lower extremities
- Difficulty with tandem gait walking
- Reduced fine motor dexterity in both hands
MRI of the cervical spine revealed severe spinal cord compression at two adjacent levels:
C5-C6 Level
Large central disc herniation causing severe cord compression with T2 signal change (myelomalacia) within the cord.
C6-C7 Level
Broad-based disc bulge and osteophytes causing moderate cord compression and severe foraminal stenosis.
Due to the severity of the cord compression and the two-level pathology, a Hybrid Surgery was recommended. This approach combines the stability of fusion with the motion preservation of arthroplasty.
C6-C7 ACDF (Fusion)
Why Fusion here? The severe spondylosis and lack of healthy facet joints made this level unsuitable for motion. Fusion ensures stability and permanent decompression.
C5-C6 Arthroplasty (Disc Replacement)
Why Replacement here? This level had relatively healthy facet joints. Preserving motion here protects the C4-C5 level above from accelerated wear (adjacent segment disease).
Timeline
Initial
Immediate relief of 'electric shock' sensations. Balance improved within 48 hours.
2 Weeks
Hand dexterity returning. Walking 5km daily. Soft collar used for comfort only.
6 Weeks
Return to office work. Started stationary cycling.
3 Months
Radiographs confirm fusion at C6-7 and mobility at C5-6. Cleared for road cycling.
Outcome Achieved
Full neurological recovery
L5–S1 Radiculopathy with Claudication
Single-Level Lumbar Arthroplasty
Susan, 54
University lecturer, Brisbane
2 Years
Progressive claudication
→ 2+ km
40-fold improvement (from 50m)
75%
ODI improvement
Patient Profile
Age / Gender
54 / Female
Occupation
University lecturer
Location
Brisbane, Queensland
Diagnosis
L5–S1 Radiculopathy with Claudication
Key Symptoms
Treatment Summary
This case demonstrates public healthcare system access to arthroplasty, extended waiting period, and dramatic functional restoration with walking tolerance improving from 50 metres to over 2 kilometres.
Demographics
- Brisbane, Queensland
- 30 years academic; primarily desk-based with some standing for teaching
Comorbidities
- Hypothyroidism (controlled)
- BMI 25 (healthy)
- Non-smoker
- DEXA T-score –0.8 (normal bone density)
Susan presented with a two-year history of progressive low back pain and left leg pain, initially attributed to sacroiliac joint dysfunction but increasingly recognised as radicular pain with claudication-like symptoms.
Public Healthcare System Pathway
Patient confirmed with public hospital that lumbar artificial disc implants available within public system. Wait time: approximately 5 months (listed January; surgery scheduled for June). Cannot select surgeon in public system; assigned to available spine surgeon.
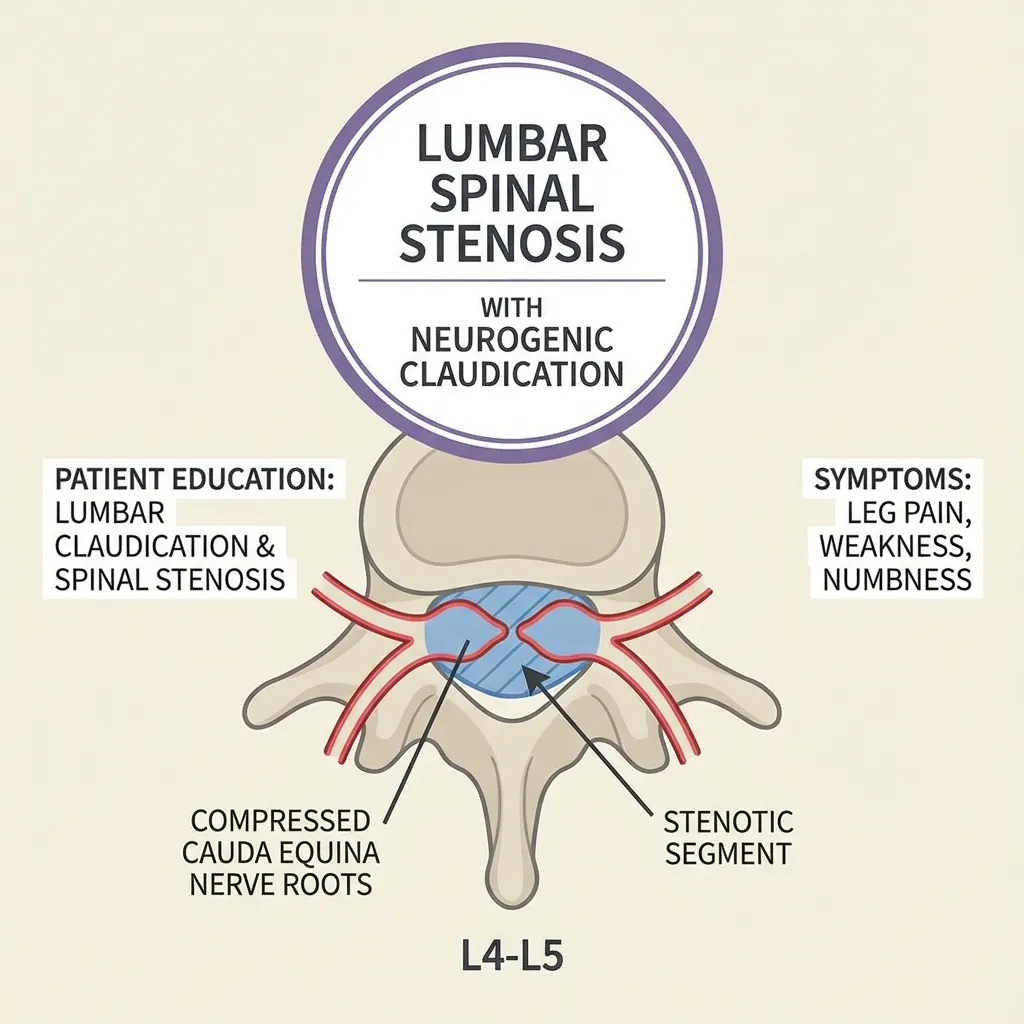
Claudication Pattern
- • Walking tolerance limited to approximately 50 metres
- • Left leg pain forces stopping; pain in calf and foot with weight-bearing
- • Symptoms resolve within 1–2 minutes of rest (sitting down)
- • Vascular assessment confirmed normal arterial circulation
- • Pain confirmed as neurogenic (not vascular) claudication
Functional Limitation
- • Unable to walk to campus shops
- • Cannot participate in family walks
- • Unable to attend standing social events
- • Severely limited participation in activities
- • Affecting quality of life and mood
Prior Conservative Care
Two years of physiotherapy; multiple courses anti-inflammatory medications; two sacroiliac joint injections (minimal benefit); epidural steroid injection at L5–S1 with temporary 4–6 week benefit, then recurrence; pain progressing to current severe limitation.
MRI Lumbar Spine
- L5–S1: Large right-sided disc herniation (extrusion) with superior migration; severe foraminal stenosis on right compressing right S1 nerve root; mild central canal stenosis
- • L4–L5: Small central disc bulge without significant stenosis
- • L3–L4: Degenerative disc changes; no stenosis
- • Facet joints: Grade 2–3 osteoarthritis at L5–S1 on right
CT Lumbar Spine with Vascular Phase
- • L5–S1 disc space: Adequate anterior vertebral body contact; endplate quality good
- • Right L5–S1 foramen narrowed approximately 50%
- • Vascular anatomy: Aorta and left iliac vessels in expected position; no aneurysm; favourable anatomy for anterior approach
Physical Examination
- • Right ankle dorsiflexion 4+/5 (slight S1 weakness)
- • Diminished sensation in right S1 distribution
- • Right Achilles reflex diminished
- • Right SLR approximately 45° (limited by leg pain)
Diagnostic Impression
Right S1 radiculopathy secondary to L5–S1 large disc herniation with foraminal stenosis, single-level disease, excellent imaging-clinical correlation.
Surgical Approach: Anterior lumbar interbody fusion (ALIF) via retroperitoneal approach at L5–S1. Surgical team included spine surgeon + vascular surgeon for vessel management and safety.
78 min
Operative Time
150 mL
Blood Loss
0
Complications
Three-Month Follow-Up Assessment
| Metric | Preoperative | 3 Months Post-op | Change |
|---|---|---|---|
| ODI Score | 56/100 (moderate-severe) | 14/100 (minimal) | 75% improvement |
| Leg Pain (VAS) | 8/10 | 0/10 | Complete resolution |
| Walking Tolerance | 50 metres | >2 km | ~40-fold improvement |
| Claudication | Severe limitation | Resolved | Complete resolution |
| Return to Work | Limited | Full duties | Achieved by week 10 |
One-Year Follow-Up
- • Sustained symptom relief: Leg pain remained completely resolved; back pain 0–1/10
- • Return to all prior activities; resumed walking for leisure; improved quality of life
- • Imaging: Stable implant, maintained disc height; segmental motion preserved (~6–7°, 85% of normal)
- • No complications; no adjacent-level symptoms developing
- • Patient stated surgery "gave me back my independence and ability to enjoy physical activities"
Clinical Significance
- Public system access to arthroplasty demonstrated
- Extended waiting period (5 months) illustrating realistic timeline
- Clear surgical indication after two years of failed conservative care
- Motion preservation at L5–S1 (highest-load segment) particularly valuable
- Vascular surgeon collaboration for safe anterior approach
- Dramatic functional restoration (50m → >2km walking)
Outcome Achieved
75% ODI improvement
L4–L5 Axial Low Back Pain Predominance
Motion Preservation at Critical Level
David, 48
Physiotherapist, Melbourne
3 Years
Exhaustive conservative care
→ 90+ min
From 30 min (3-fold improvement)
73%
Disability reduction
Patient Profile
Age / Gender
48 / Male
Occupation
Physiotherapist
Location
Melbourne
Diagnosis
L4–L5 Axial Low Back Pain
Key Symptoms
Treatment Summary
This case illustrates axial pain relief through disc replacement, biomechanical rationale for motion preservation at L4–L5 (critical load-bearing segment), and long-term adjacent segment protection.
David presented with a three-year history of progressive L4–L5 axial low back pain, initially attributed to occupation-related strain but increasingly recognised as degenerative disc disease.
Occupation
20 years healthcare; significant standing, bending, and patient handling
Pain Characteristics
- • Central lower lumbar pain, worse with standing, bending, patient lifting
- • Radiates into bilateral lower back and gluteal regions (referred, non-radicular)
- • Baseline 5–6/10, worsens to 8–9/10 with activity
Functional Impact
- • Unable to stand for teaching (previously 2–3 hour lectures now limited to 30 minutes)
- • Unable to perform clinical patient handling
- • Avoided recreational activities (previously active in sport)
Conservative Treatment
- • 3 years physiotherapy, anti-inflammatory medications
- • 3 epidural steroid injections (2–4 week benefit each)
- • Diminishing return with each injection
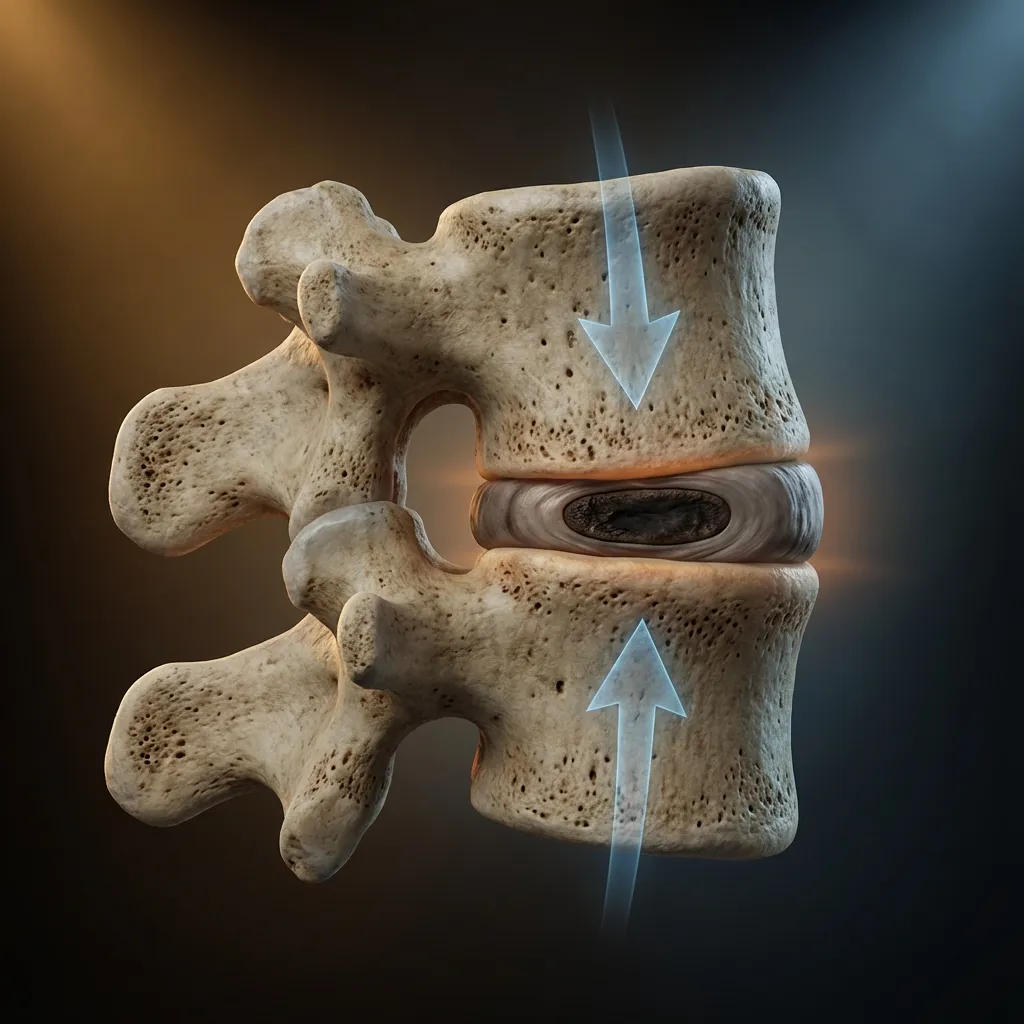
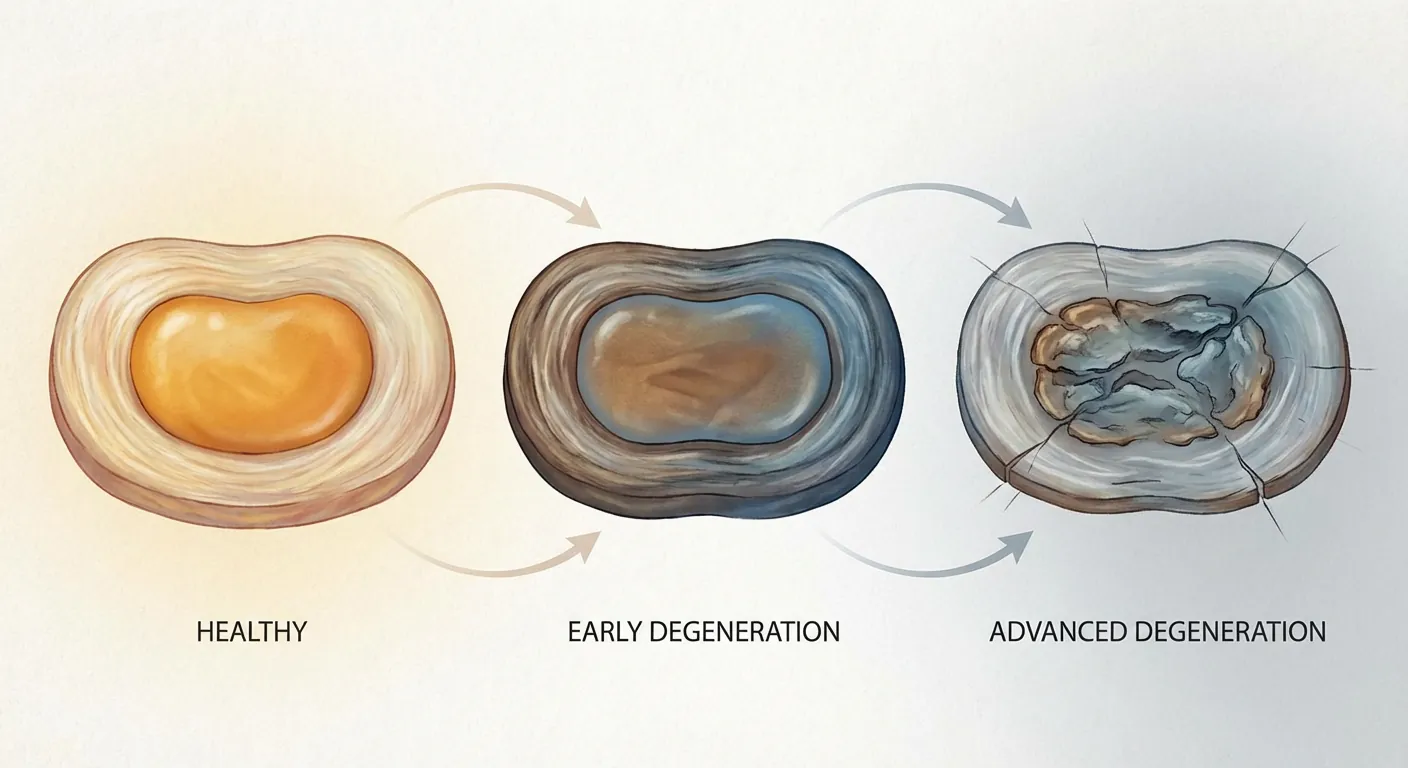
Understanding Load Distribution in Lumbar Spine
The lumbar spine functions as a load-bearing structure where each segment shares responsibility for supporting axial loads from body weight, gravity, and dynamic movements. Normal lumbar disc height and segmental motion distribute loads physiologically across nucleus pulposus and annulus fibrosus.
David's Imaging Findings
- • Reduced disc height (~8 mm vs normal 11–12 mm; ~25% height loss)
- • Loss of nucleus pulposus signal (dehydration indicating collagen disruption)
- • Reduced elasticity and load-distribution capacity
Intradiscal Pressure Changes
- • L4–L5 experiences 30% increase in intradiscal pressure during flexion
- • Up to 80% pressure increase during extension
- • Explains David's functional limitation
Motion Preservation Benefits at L4–L5
- Restored load distribution: More physiological pressure distribution across nucleus and annulus
- Adjacent segment protection: Maintained L4–L5 motion prevents compensatory stress transfer to L3–L4 and L5–S1
- Proprioceptive feedback: Preserved motion maintains normal spinal proprioception and motor control
- Long-term occupational capacity: Motion preservation allows David to continue physically demanding occupation
Fusion Disadvantage (Biomechanical)
Rigid L4–L5 fusion would eliminate approximately 8–10° segmental motion, forcing adjacent segments (L3–L4 and L5–S1) to compensate with increased motion and loading. Research demonstrates that within 5–10 years, this compensatory stress accelerates degeneration at adjacent levels—exactly the problem fusion was supposed to solve.
MRI Lumbar Spine
- L4–L5: Pfirrmann Grade 3–4 degeneration; reduced disc space height; loss of T2 signal in nucleus pulposus; central disc bulge causing mild compression
- • L3–L4: Mild degenerative changes; adequate disc height
- • L5–S1: Mild degenerative changes; adequate disc height
- • Facet joints: Grade 1–2 at L4–L5 (mild)
Provocative Discography
Given predominance of axial pain and lack of clear radicular features, discography was performed as diagnostic adjunct:
- • L4–L5: Injection reproduced familiar axial pain at low volumes (positive test)
- • L3–L4: No pain (negative control)
- • L5–S1: No pain (negative control)
Diagnostic Impression
L4–L5 discogenic low back pain (axial pain predominance) secondary to degenerative disc disease, with failure of conservative management over three years. Excellent candidate for motion-preserving lumbar disc replacement at L4–L5 level.
72 min
Operative Time
120 mL
Blood Loss
+25%
Disc Height Restored
Three-Month Follow-Up Assessment
| Metric | Preoperative | 3 Months | Significance |
|---|---|---|---|
| ODI Score | 44/100 (moderate) | 12/100 (minimal) | Exceeds MCID (10–15 points) |
| Back Pain (VAS) | 6/10 | 2/10 | Clinically significant |
| Referred Pain (bilateral gluteal) | 5/10 | 0/10 | Complete resolution |
| Standing Tolerance | 30 minutes | 90+ minutes | 3-fold improvement |
| Satisfaction | N/A | 88/100 | Highly satisfied |
One-Year Follow-Up
- • Sustained pain relief: Axial low back pain maintained at 1–2/10; no recurrence of referred gluteal pain
- • Able to perform all occupational duties including patient handling
- • Resumed recreational sports participation (running, recreational football)
- • Imaging: Segmental motion preserved (~7–8°, 85–90% of normal L4–L5 motion)
- • Patient stated surgery "restored my capacity to function as a physiotherapist and return to the activities I loved"
Clinical Significance
- Axial pain relief: Disc replacement effective for axial low back pain when disc-related
- Load distribution restoration: Restoring disc height re-establishes physiological pressure distribution
- Long-term protection: Motion preservation at L4–L5 protects adjacent segments
- Aging beneficially: At age 48, preserving motion for next 30–40 years substantially beneficial
Outcome Achieved
73% ODI improvement
L5–S1 with Grade 1 Anterolisthesis
Motion Preservation Despite Mild Instability
Michelle, 56
School administrator, Brisbane
18 Months
Progressive right leg pain
→ 2+ km
From 100m (~20-fold improvement)
92/100
Highly satisfied
Patient Profile
Age / Gender
56 / Female
Occupation
School administrator
Location
Brisbane
Diagnosis
L5–S1 with Grade 1 Anterolisthesis
Key Symptoms
Treatment Summary
This case illustrates that Grade 1 anterolisthesis is not a contraindication to disc replacement and demonstrates excellent outcomes at the most load-bearing lumbar level.
Michelle presented with an 18-month history of progressive right lower leg pain severely limiting her walking capacity and quality of life.
Claudication Pattern
- • Can walk approximately 100 metres before pain forces stopping
- • Pain localised to calf and foot
- • Symptoms resolve within 1–2 minutes of sitting (standing relief not sufficient)
- • Baseline 3–4/10 at rest; 8–9/10 with walking
Conservative Management
- • 18 months physiotherapy with minimal benefit
- • Multiple courses neuropathic medications (pregabalin, duloxetine)
- • Two epidural steroid injections (diminishing response)
- • Ankle-brachial index normal (vascular cause excluded)
Michelle's imaging revealed slight anterolisthesis (Grade 1; approximately 2–3 mm). This raised the question: Does it preclude disc replacement?
Anterolisthesis Grading
Grade 1
<25% translation
Michelle's case
Grade 2
25–50%
Relative contraindication
Grade 3
50–75%
Contraindication
Grade 4
>75%
Contraindication
Michelle's Assessment
- • ~3 mm in ~33 mm vertebral body = ~9% translation
- • Well within Grade 1 (minimal)
- • Dynamic X-rays: No excessive motion
- • Facet arthritis providing passive stability
Conclusion
Grade 1 anterolisthesis was not a contraindication to disc replacement. Arthroplasty can actually restore stability through height restoration and improved segmental mechanics.
MRI Lumbar Spine
- L5–S1: Large right-sided disc herniation (extrusion with superior migration); right L5–S1 foramen severely narrowed; right S1 nerve root clearly compressed
- • Facet joints: Grade 2–3 osteoarthritis at L5–S1 (more prominent on right)
- • L4–L5: Small central disc bulge without significant stenosis
CT with Vascular Phase
- • Right L5–S1 foramen narrowed approximately 60%
- • Vascular anatomy: Left-sided retroperitoneal approach optimal and safe
80 min
Operative Time
160 mL
Blood Loss
Immediate
Leg Pain Relief
| Metric | Preoperative | 3 Months | Change |
|---|---|---|---|
| ODI Score | 52/100 | 16/100 | 69% improvement |
| Leg Pain | 8–9/10 | 0/10 | Complete resolution |
| Walking Tolerance | 100 metres | 2+ km | ~20-fold improvement |
| Motor Strength | 4+/5 | 5/5 | Normalised |
Adjacent-Segment Assessment at 1 Year
L4–L5 (which demonstrated early degenerative changes preoperatively) remained stable without progression; motion preserved at L4–L5. This demonstrates that motion preservation at L5–S1 protects the adjacent segment.
Clinical Significance
- L5–S1 motion preservation critically important at highest load-bearing level
- Grade 1 anterolisthesis compatible with successful disc replacement
- Complete claudication relief from anterior decompression
- Adjacent-segment protection demonstrated at follow-up
- Superior long-term outcomes with disc replacement vs fusion at L5–S1
Outcome Achieved
92/100 Satisfaction
Hybrid Lumbar Surgery
L5–S1 ALIF + L4–L5 Disc Replacement

Robert, 62
Retired business owner, Sydney
Two-Level
L4–L5 and L5–S1 disease
→ 2+ km
From 200m (~10-fold improvement)
67%
Disability reduction
Patient Profile
Age / Gender
62 / Male
Occupation
Retired business owner
Location
Sydney
Diagnosis
Two-Level Lumbar Degeneration
Key Symptoms
Treatment Summary
This case demonstrates pathology-specific treatment matching — fusion at the severely degenerated level with arthroplasty at the moderately affected level above.
Robert presented with a two-year history of progressive bilateral low back pain and bilateral leg pain affecting quality of retirement and family activities.
Symptoms
- • Central and bilateral lower lumbar pain (5–6/10 baseline, 8–9/10 with activity)
- • Bilateral leg pain: Right 7–8/10, left 4–5/10
- • Both radiating into calves
- • Walking limited to 100–200 metres
Functional Impact
- • Previously active in golf, walking, travel
- • Unable to pursue leisure activities
- • Affecting retirement quality significantly
L5–S1 Findings
- • Severe degenerative changes (Pfirrmann Grade 4)
- • Large bilateral disc herniation
- • Bilateral foraminal stenosis
- • Grade 3–4 facet arthritis
- • Disc height only ~7 mm (severely reduced)
- → Arthroplasty alone may not address facet pathology
L4–L5 Findings
- • Moderate degenerative changes (Pfirrmann Grade 3)
- • Mild-to-moderate central disc bulge
- • Disc height ~10 mm (moderately reduced)
- • Grade 2 facet arthritis
- → Suitable for motion-preserving arthroplasty
Surgical Options Comparison
Eliminates motion at two levels; adjacent-segment disease risk 40–50% at 10 years
L5–S1 facet arthritis may compromise long-term success; technically challenging
Fusion addresses severe L5–S1 facet arthritis; arthroplasty preserves motion at L4–L5; best of both approaches
Key Biomechanical Advantage
By preserving L4–L5 motion, hybrid procedure protected L3–L4 from compensatory stress. One-year follow-up showed L3–L4 maintained preoperative motion without increase — confirming that the hybrid construct did not create compensatory stress transfer to the next level above.
105 min
Operative Time
200 mL
Blood Loss
Bilateral
Leg Pain Relief
| Metric | Preoperative | 3 Months | Change |
|---|---|---|---|
| ODI Score | 54/100 | 18/100 | 67% improvement |
| Right Leg Pain | 8/10 | 0/10 | Complete resolution |
| Left Leg Pain | 5/10 | 0/10 | Complete resolution |
| Walking Tolerance | 100–200 metres | 2+ km | ~10-fold improvement |
| Golf Participation | Unable | Full rounds | Quality of life restored |
One-Year Imaging
- • L5–S1: Solid fusion (bone incorporation visible on X-rays)
- • L4–L5: Stable disc replacement with motion preserved (~6–7°)
- • L3–L4: Stable motion (preoperative motion maintained; no compensatory increase)
Clinical Significance
- Pathology-specific treatment: Severe level gets fusion; moderate level gets arthroplasty
- Avoiding over-fusion: Maintains motion where it's still beneficial
- Adjacent segment protection: L4–L5 motion protects L3–L4
- Long-term superiority: Superior outcomes vs two-level fusion in literature
Outcome Achieved
67% ODI improvement
When Things Get ComplexManaging Real-World Challenges
These cases demonstrate how complications and complex scenarios are identified and managed — addressing adjacent-level disease after prior fusion and handling postoperative complications with successful resolution.
Adjacent-Level Disease After Prior Fusion
Anthony, 54
Engineer, Perth
Prior L5–S1 PLIF
8 years ago
Current: L4–L5
Adjacent segment disease
L4–L5 TDR
Motion-preserving revision
Anthony underwent L5–S1 fusion eight years ago with initial good results. Over the past 18 months, he developed progressive L4–L5 symptoms — a classic presentation of adjacent segment disease.
Current Presentation
- • Central low back pain radiating into bilateral gluteal regions
- • Mild right-sided radiculopathy (L4 distribution)
- • Walking tolerance reduced to 500m (was 2+ km)
- • MRI: L4–L5 moderate stenosis, disc herniation
Treatment Decision
- • Option A: Extend fusion to L4 (lose more motion)
- • Option B: L4–L5 disc replacement
- • Chosen approach preserves remaining lumbar motion
- • Protects L3–L4 from becoming the next "adjacent segment"
70 min
Operative Time
500m → 2+ km
Walking Tolerance
65%
ODI Improvement
Key Lesson
Disc replacement above prior fusion can be successful and may protect against further propagation of the "domino effect" (cascade of adjacent segment disease). One-year imaging showed L3–L4 remained stable.
Complication — Postoperative Hematoma
Thomas, 63
Retired tradesman, Adelaide
L5–S1 Arthroplasty
Initial procedure
Hematoma Day 2
Complication identified
Excellent Recovery
After management
This case illustrates that while complications are uncommon, they can occur, and early recognition with appropriate intervention leads to successful outcomes.
Day 2 Postoperative Event
- • Progressive abdominal pain and distension
- • Mild tachycardia (heart rate ~100)
- • Haemoglobin dropped from 135 to 105 g/L
- • CT scan: Moderate retroperitoneal haematoma anterior to L5–S1
Management
- • Multidisciplinary review (vascular surgery, ICU)
- • Conservative approach: observation, blood transfusion (2 units PRBC)
- • Serial examinations, repeat imaging
- • Haematoma remained stable → resolved over 2 weeks
Outcome
- • Extended hospital stay (5 days total)
- • Full recovery by discharge
- • Three-month follow-up: Excellent symptom relief
- • Patient satisfied despite complication
Detection
- Regular post-op monitoring protocols
- Early symptom recognition
- Prompt imaging when concerned
Management Principles
- Multidisciplinary input (vascular, ICU, surgeon)
- Conservative approach when stable
- Serial monitoring until resolution
Key Takeaway
Complications, while uncommon (~1–2% require intervention for spinal arthroplasty), can occur with any surgical procedure. What matters is: early recognition, appropriate response, multidisciplinary collaboration, and transparent patient communication. Thomas ultimately had an excellent outcome despite the complication.
Complex Scenario Insights
- Adjacent segment disease is predictable after fusion — arthroplasty can address it
- Disc replacement above existing fusion can break the "domino effect"
- Complications require early recognition and appropriate management
- Most complications resolve with conservative management
Patterns from These CasesWho Benefits Most?
These eight cases reveal consistent patterns in patient selection and decision-making. The following criteria summarise what makes an ideal arthroplasty candidate versus when fusion may be preferable.
Ideal Arthroplasty Candidate
All cases demonstrated these characteristics
- Single or two-level disease with clear imaging-clinical correlation
- Failure of adequate conservative care (minimum 6 weeks to 6 months)
- Predominant axial or radicular (not facet) pain pattern
- Adequate bone quality on imaging (no severe osteoporosis)
- Mild-to-moderate facet joint arthritis (Grade 1–2)
- Preserved segmental motion on dynamic imaging
- Active lifestyle and long life expectancy (younger patients)
- Clear patient understanding of risks and realistic expectations
- No spinal instability exceeding Grade 1 spondylolisthesis
- Favourable vascular anatomy for anterior approach (lumbar)
When Fusion May Be Preferable
Relative or absolute contraindications
- Severe facet joint arthritis (Grade 3–4)
- Significant spinal instability (Grade 2+ spondylolisthesis)
- Multi-level deformity requiring correction
- Severe osteoporosis (T-score < –2.5)
- Active spinal infection
- Severe multi-level disease (3+ levels)
- Unfavourable vascular anatomy (lumbar)
- Previous major abdominal surgery with adhesions
Note: These are relative considerations, not absolute rules. Case 5 (Grade 1 anterolisthesis) and Case 6 (L5–S1 with facet arthritis treated with fusion + L4–L5 arthroplasty) demonstrate nuanced decision-making.
Surgical Options Comparison
| Factor | Disc Replacement | Fusion |
|---|---|---|
| Motion Preservation | Yes (85–90%) | No |
| Adjacent Segment Disease Risk (10 yr) | 5–15% | 25–35% |
| Return to Activity | Typically faster (no fusion needed) | Slower (fusion consolidation) |
| Handles Severe Facet Arthritis | Limited | Yes |
| Handles Instability | Grade 1 only | All grades |
| Best For | Younger, active patients with disc pathology | Instability, severe facet disease, deformity |
The goal is not to choose arthroplasty over fusion universally — it's to match the right treatment to the right patient based on their specific pathology, anatomy, and goals.
Recovery TimelinesWhat to Expect
Based on these case studies and broader clinical experience, here are the typical recovery milestones for cervical and lumbar arthroplasty.

Early Recovery
Weeks 2–4
Cervical Arthroplasty
- Wean soft collar by week 2–3
- Light activities resume
- Driving at 2–3 weeks (neck mobility check)
- Return to desk work possible
Lumbar Arthroplasty
- Walking tolerance increasing
- Gentle stretching begins
- Standing/sitting time increasing
- No lifting >5 kg
Note: These timelines represent typical progression. Individual recovery varies based on age, fitness, surgical complexity, and adherence to rehabilitation protocols. Always follow your surgeon's specific guidance.
What These Cases Teach UsKey Factors for Success

Careful Patient Selection
Matching pathology to treatment approach — arthroplasty for disc disease, fusion for instability/facet arthritis
Imaging-Clinical Correlation
Clear match between symptoms, examination findings, and imaging abnormalities
Adequate Conservative Trial
Minimum 6 weeks to 6 months of non-surgical treatment before surgery
Technical Proficiency
Precise implant positioning and complete decompression of neural structures
Realistic Expectations
Patients understanding that surgery addresses structural pathology, not all pain sources
Structured Rehabilitation
Appropriate post-operative care and gradual return to activity
Long-Term Follow-Up
Monitoring for complications, adjacent segment changes, and sustained function
Case Study Summary
Cases 1–2 (Cervical): Single and two-level arthroplasty with excellent radicular and myelopathy outcomes
Cases 3–5 (Lumbar): L5–S1 claudication relief, axial pain resolution, anterolisthesis compatibility
Case 6 (Hybrid): Pathology-specific treatment matching with fusion + arthroplasty
Cases 7–8 (Complex): Adjacent segment disease management and successful complication resolution
The Fundamental Lesson
Arthroplasty is not a universal solution — it's a precise tool for specific indications. When patients are carefully selected and procedures technically well-performed, outcomes are consistently excellent.
The key is matching the right treatment to the right patient, with realistic expectations and appropriate follow-up.
If you're experiencing symptoms similar to these case studies, consider consulting a spine specialist to discuss whether arthroplasty may be appropriate for your situation.
Learn More About Patient Evaluation