
Cervical Spine Anatomy Anatomical Foundation
Detailed exploration of cervical spine anatomy, the seven vertebrae, neural architecture, and biomechanical function. Understanding normal cervical anatomy is essential for appreciating how disc replacement surgery restores optimal function and eliminates chronic neck pain.
Cervical Support
Structural Framework
7 Vertebrae
Seven cervical vertebrae (C1-C7) providing critical support for the head while enabling the widest range of motion in the entire spine.
Neural Pathways
Spinal Cord Protection
Critical
Critical neural pathways including the spinal cord and nerve roots requiring precise anatomical understanding for safe surgical intervention.
Range of Motion
Biomechanical Detail
Dynamic
Sophisticated biomechanical design allowing complex head movements including rotation, flexion, extension, and lateral bending.
The Cervical Spine Architecture
The cervical spine is not just a stack of bones. It is a precise mechanical system designed for stability, protection, and mobility.
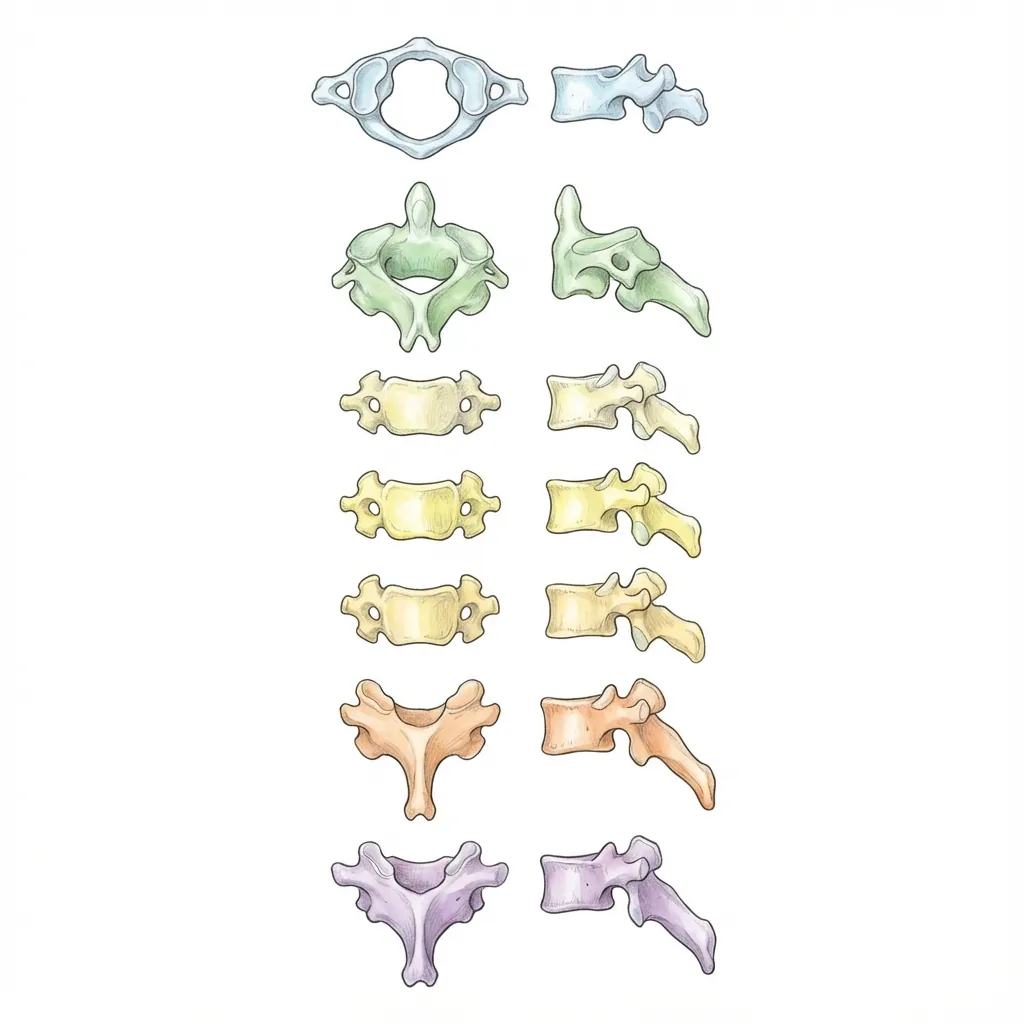
The Seven Guardians
Click levels to explore each vertebra
C1 (Atlas)
Named after the titan Atlas who held the heavens. Your C1 supports your skull—about 10 pounds of weight—and allows your head to nod up and down (flexion-extension).
Key Features
- Ring-like structure without a central body
- Two lateral masses articulating with skull above and C2 below
- Enables nodding "yes" motion
Vertebral Body Engineering
Each cervical vertebra (C3-C7) contains a vertebral body—the cylindrical, load-bearing portion anterior (front) of the spine.
17-20mm
16-18mm
80%
Primary
Clinical Significance: The vertebral bodies are where osteoporosis affects the cervical spine. Adequate bone quality is essential for implant stability during arthroplasty.
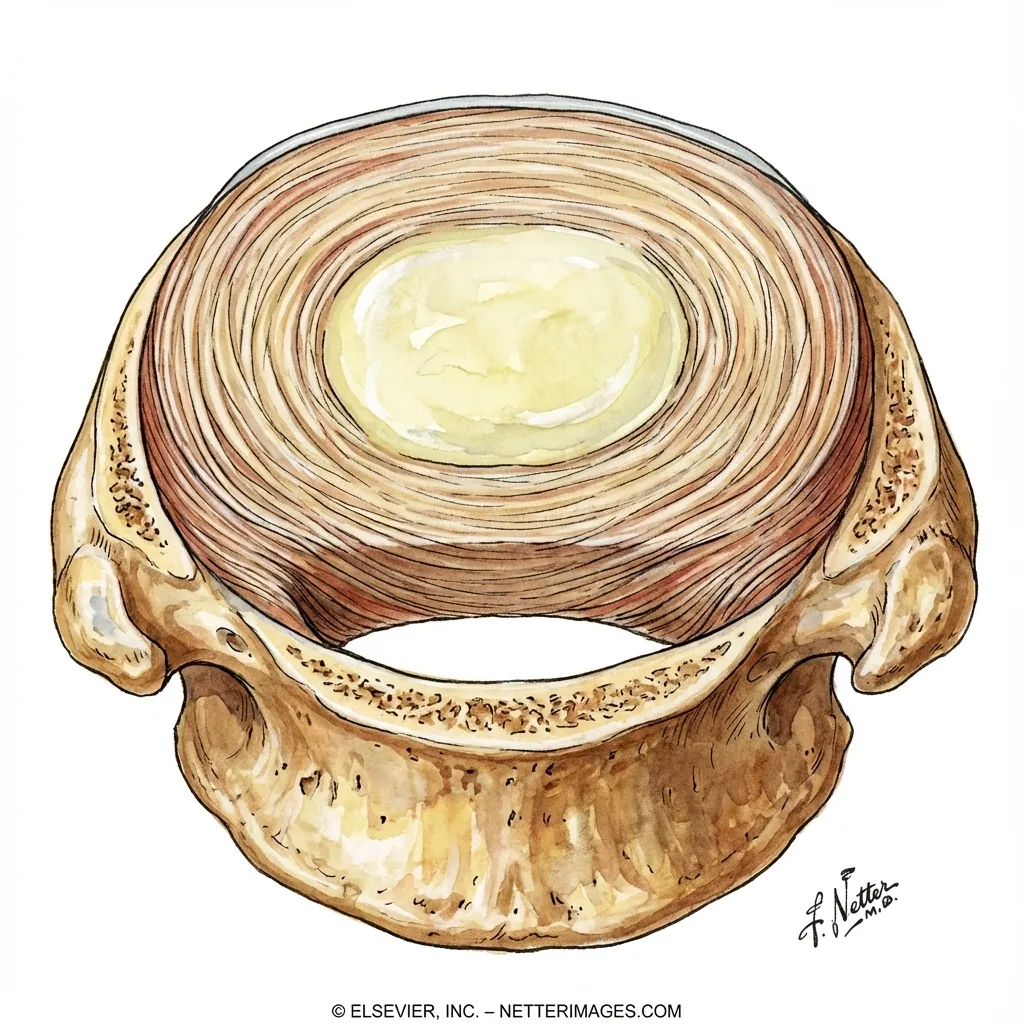
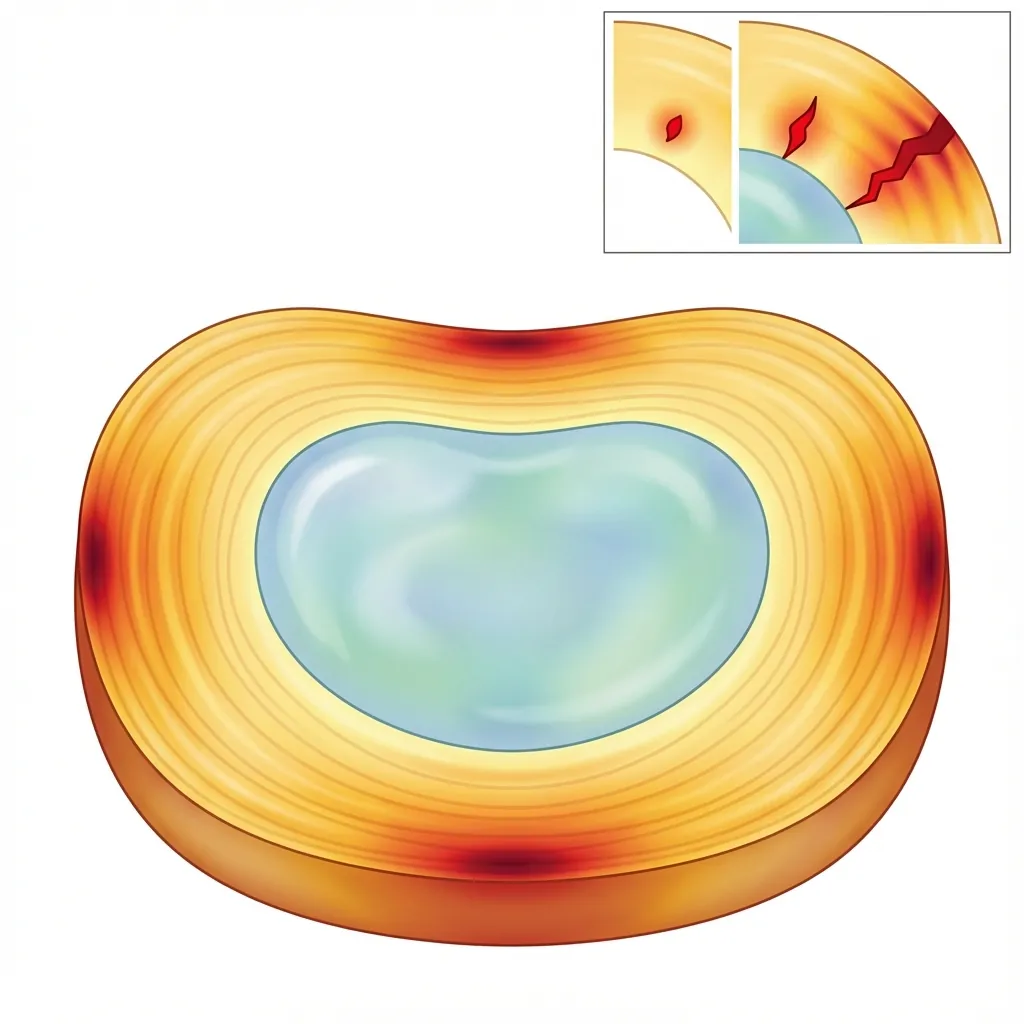
The Intervertebral Disc
Between each vertebral body sits an intervertebral disc—one of nature's most elegant engineering solutions. These discs serve three critical functions: load-bearing, shock absorption, and mobility allowance.
Nucleus Pulposus
The gel-like inner core—nature's hydraulic cushion.
- Water content: 80-90% in healthy young discs
- Proteoglycans attract and hold water
- Type II collagen provides structural framework
- Creates turgor pressure for shock absorption
Pedicles
Short pillars connecting anterior and posterior structures
Laminae
Thin plates forming the posterior wall of the vertebral canal
Spinous Processes
Bony projections (the bumps you feel down your neck)
Facet Joints
Synovial joints that guide motion and share 20-25% of compressive load
The Neural Architecture
Protected within the bony canal lies the body's most sensitive communication network—the spinal cord and its branching nerve roots.

The Spinal Cord
The Information Highway
Running through the centre of the vertebral canal is the spinal cord—a continuation of the brainstem that terminates around the L1 vertebra in adults. The cervical cord is divided into 8 cervical segments (C1-C8), each giving rise to spinal nerve roots.
Composition
Central butterfly-shaped nerve cell bodies
Outer myelinated axons (signal pathways)
The Critical Passage
The intervertebral foramen is where nerve roots exit the spine—and where they are most vulnerable to compression from disc herniation, bone spurs, or ligament thickening.
6-8mm
Quite narrow
40-50%
Limited reserve space
Protective Layers (Meninges)
The spinal cord floats in cerebrospinal fluid (CSF) and is wrapped in three protective membranes.
Tough, fibrous outer layer forming a protective sac
Middle web-like structure
Delicate inner layer directly attached to cord
Nerve Root Functions
Each nerve root serves specific muscles and skin areas—this is why doctors can pinpoint your injury by asking where you feel pain.
Elbow flexion, wrist extension
Thumb, index finger, lateral forearm
Forearm pain, thumb numbness
Diminished biceps reflex
Radiculopathy
Pinched Nerve Root
Occurs when disc herniation or bone spurs compress the nerve root exiting the spine. Often resolves without surgery (90% of cases).
- Unilateral (one-sided) symptoms
- Pain radiates down the arm in specific path
- Numbness in specific fingers
- Weakness in specific muscles
Myelopathy
Spinal Cord Compression
A much more serious condition where the main spinal cord itself is compressed. Can cause progressive, potentially irreversible neurological damage.
- Bilateral symptoms (both sides)
- Gait disturbance, balance problems
- Hand clumsiness, fine motor difficulty
- URGENT: Requires surgical evaluation
Ligaments & Biomechanics
The "Soft Skeleton" that holds everything together and orchestrates the elegant dance of cervical movement.
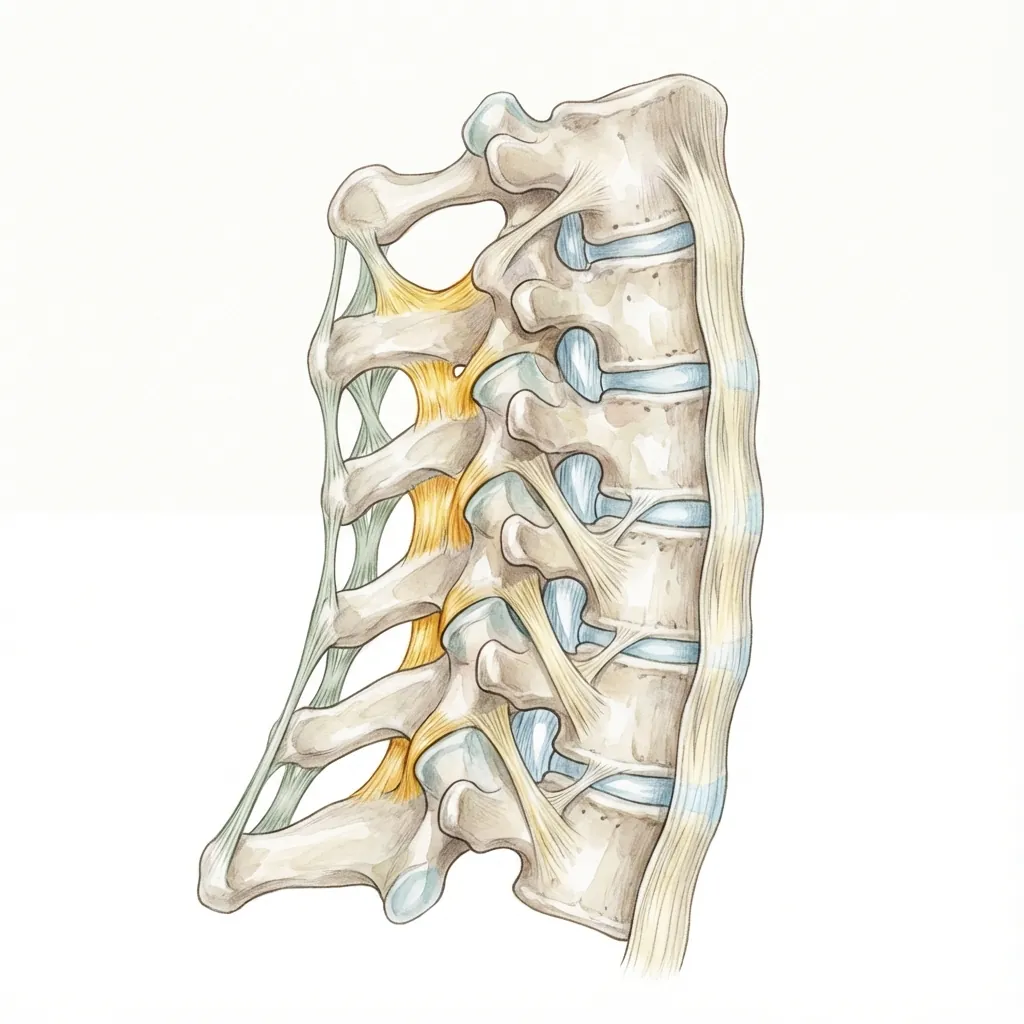
Anterior Longitudinal Ligament (ALL)
Runs along the anterior surface of vertebral bodies
Prevents excessive extension (backward bending)
1.5-2mm — one of the strongest spinal ligaments
Limits disc material anteriorly, so most herniations occur posteriorly
Healthy Ligament Properties
Can stretch and return to original length
Responds differently to fast vs. slow loading
Resists tensile forces
Provides position and movement feedback
Degenerative Changes
- Loss of elasticity → increased rigidity
- Hypertrophy (thickening) → narrowed canal
- Calcification → further rigidity
- Loss of water content → reduced shock absorption
Biomechanical Function
The cervical spine permits six degrees of freedom—movement in three planes with remarkable precision and control.
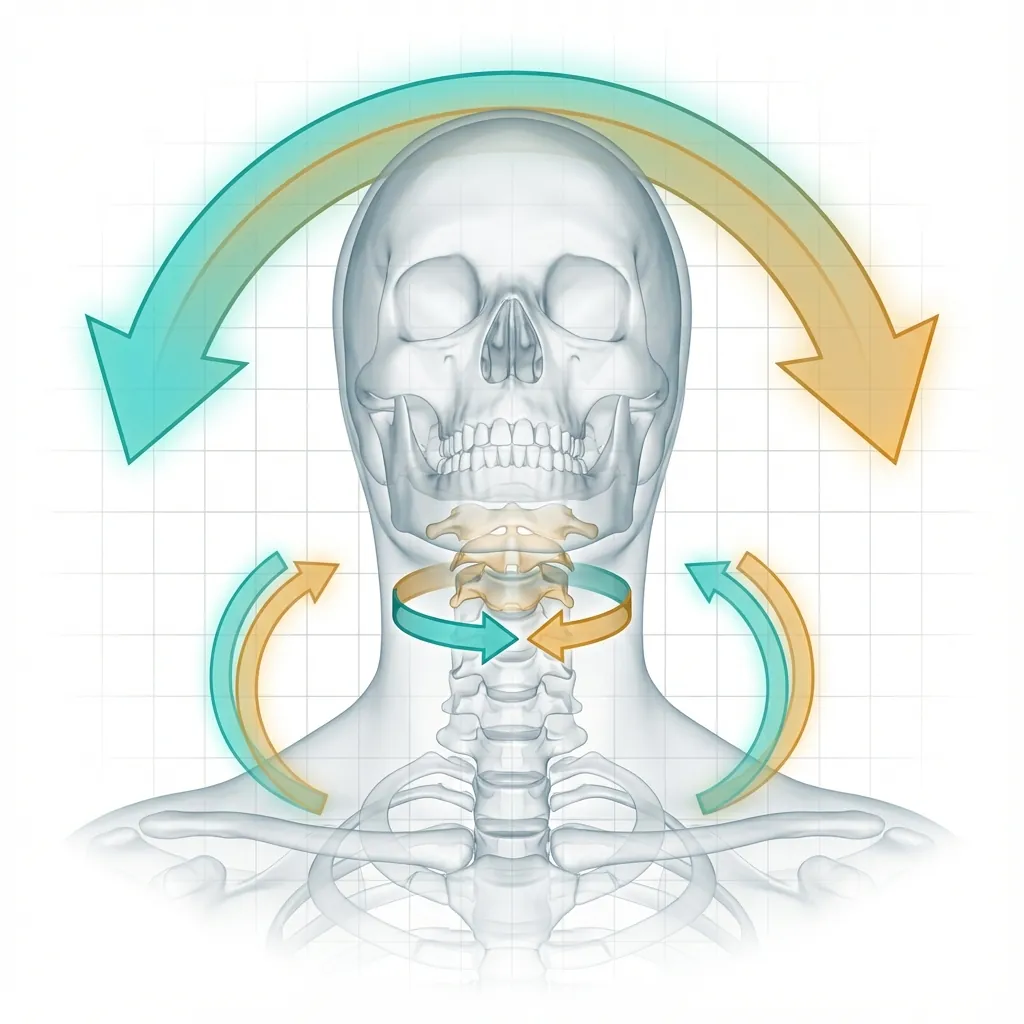
Flexion-Extension
Forward and backward bending primarily at C4-C5 and C5-C6.
Total Range: 130-160°Lateral Flexion
Side-to-side bending, coupled with rotation at each level.
Range: 20-45° per sideRotation
C1-C2 accounts for ~50% of total cervical rotation (45° each side).
Total Range: 70-90°Load Distribution
The Neutral Zone
The range of motion under low load before ligaments become load-bearing. In healthy spines, this zone is small (tight ligaments). In degenerative spines, the zone enlarges (lax ligaments), causing instability and pain.
Coupled Movements
The cervical spine exhibits coupled motion patterns—movements that occur together due to anatomy. For example, flexion couples with contralateral rotation and lateral flexion. These patterns are built into the facet joint orientation and disc fibre angles.
Biomechanical Loading & Stress
Understanding how daily activities affect disc pressure explains why posture matters—and how degeneration accelerates.
Similar to standing
Daily Activities & Disc Pressure
Posture Impact: Persistent forward head posture (common with device use) increases disc pressure and accelerates degeneration over time.
Stress Concentration & Progressive Failure
In a degenerating disc, stress redistributes in a cascade that accelerates damage—like a tire with a small puncture that progressively weakens.
Early Degeneration
Nucleus loses water and becomes stiffer
Pressure Increase
Remaining nucleus experiences higher pressure concentrations
Annular Stress
Increased loads transmit to outer annulus fibres
Annular Fissures
High localised stresses cause microruptures in fibres
Progressive Herniation
Fissures enlarge; nucleus material herniates through
Acceleration
Degeneration accelerates as pathological loading increases
The Tire Analogy: Imagine a tire with a small puncture. The initial puncture doesn't cause immediate failure, but the stress concentration at the puncture site makes the tire progressively weaker until catastrophic failure occurs.
Segmental Instability
When discs degenerate, segmental instability develops—excessive shear translation between adjacent vertebrae that triggers a positive feedback loop of progressive degeneration.
Instability Mechanism
Clinical Symptoms
Positional, activity-dependent
Audible sensations during movement
"Giving way" sensation
Acute flares with minor triggers
How Arthroplasty Restores Anatomy
Spinal arthroplasty addresses the fundamental problem: restoring load-bearing, shock-absorbing, and motion-preserving disc function.
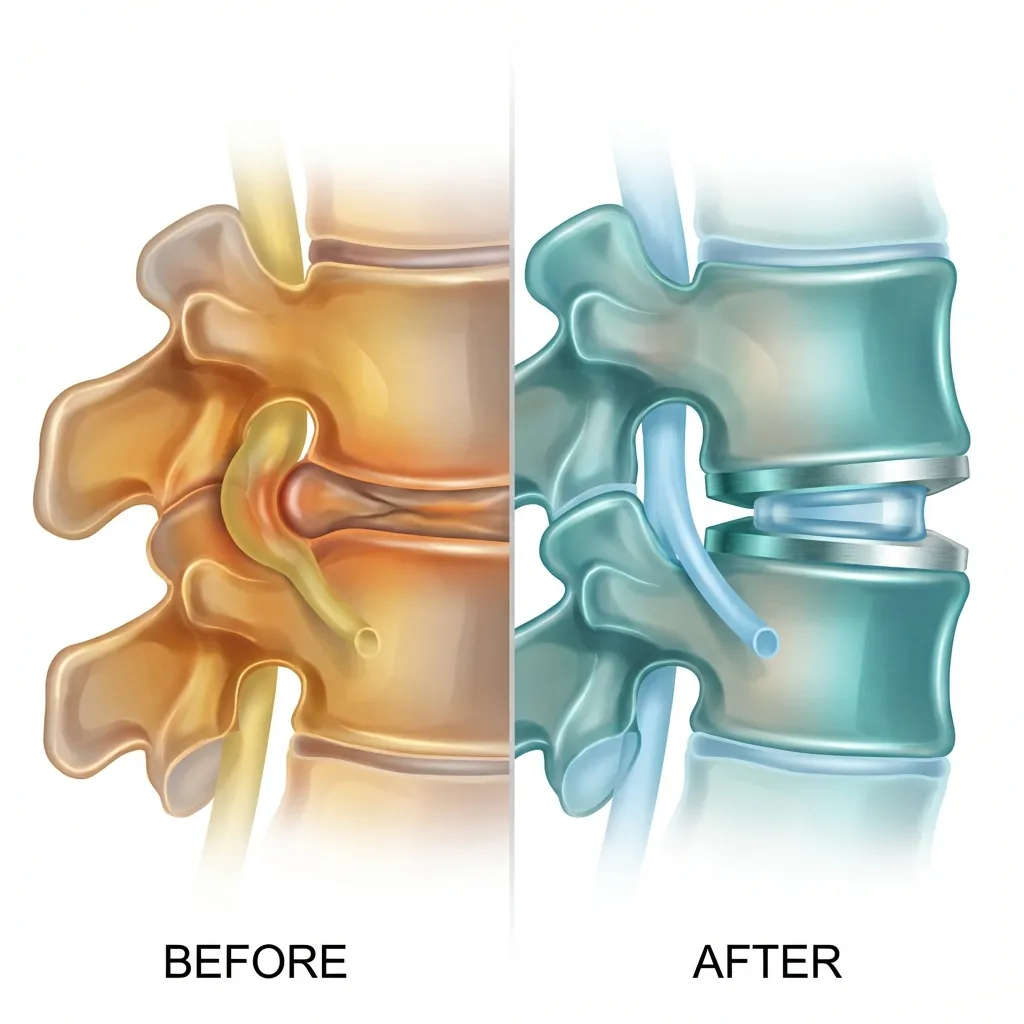
The Engineering Solution
Artificial disc replacement restores the three critical functions of a healthy disc: load distribution, controlled motion, and adjacent segment protection.
- • Collapsed disc height
- • Compressed nerve root
- • Painful instability
- • Restored disc height
- • Decompressed foramen
- • Preserved motion
Disc Height Restoration
2-3mm (collapsed)
5-6mm (normal)
- Opens intervertebral foramina → decompresses nerve roots
- Restores segmental lordosis (natural curve)
- Reduces facet joint compression
- Normalises ligament tension
Load-Bearing Function
Failed hydraulic cushion
Metal endplates + polymer core
- Provides stiff, load-bearing surface
- Prevents vertebral endplate subsidence
- Distributes forces appropriately
- Achieves same decompression as fusion
Motion Preservation
Painful, unstable motion
6-8° controlled movement
- Maintains segmental kinematics
- Reduces compensatory motion at adjacent segments
- Allows limited rotation (2-4°)
- Cumulative adjacent-segment protection
Adjacent Segment Protection
Progressive wear cascade
Physiological load distribution
- Distributes load more physiologically
- Reduces adjacent-segment stress
- Lower reoperation rates at 20-30 years
- Sustained preservation vs fusion
Why 20+ Years Matters
The true advantage of motion preservation emerges over decades, not months. Here's how outcomes diverge over time.
| Timeframe | Fusion | Arthroplasty |
|---|---|---|
| Year 1-5 | Both work well | Both work well |
| Year 5-15 | ASD begins (25-30%) | Continued preservation |
| Year 15-30 | New symptoms develop | Sustained outcomes |
| Year 30+ | Higher reoperation | Lower reoperation |
Key Insight: Both procedures achieve excellent short-term results. The arthroplasty advantage compounds over decades through adjacent segment protection.
The Degenerative Cascade
Spinal ageing isn't random. It follows a predictable cascade described by Kirkaldy-Willis. Understanding where you are in this timeline is the first step to treatment.

Stage 1: Silent Changes
Proteoglycan loss from nucleus, decreased water content, and altered collagen organisation. The disc is still maintaining height.
Clinical Presentation
- Asymptomatic
- No pain yet
- Subtle cellular changes
Imaging Findings
Normal or minimal changes on MRI
Intervention Window
Prevention focus—posture, ergonomics, exercise
Optimal Window: Early intervention prevents progression to later stages.
Why Intervention Timing Matters
Early Intervention (Stage 2-3)
- Prevents progression to Stages 4-5
- Restores disc anatomy before irreversible facet changes
- Maintains long-term spinal motion and function
- Avoids need for future revision surgeries
Delayed Intervention (Stage 4-5)
- May not be candidate for arthroplasty
- May require fusion instead (less motion preservation)
- Higher risk of adjacent-segment surgeries
- Significant facet arthritis often contraindicates arthroplasty
Clinical Anatomy & Symptoms
Why your symptoms correlate to specific levels—and how surgeons use this knowledge for precise diagnosis.
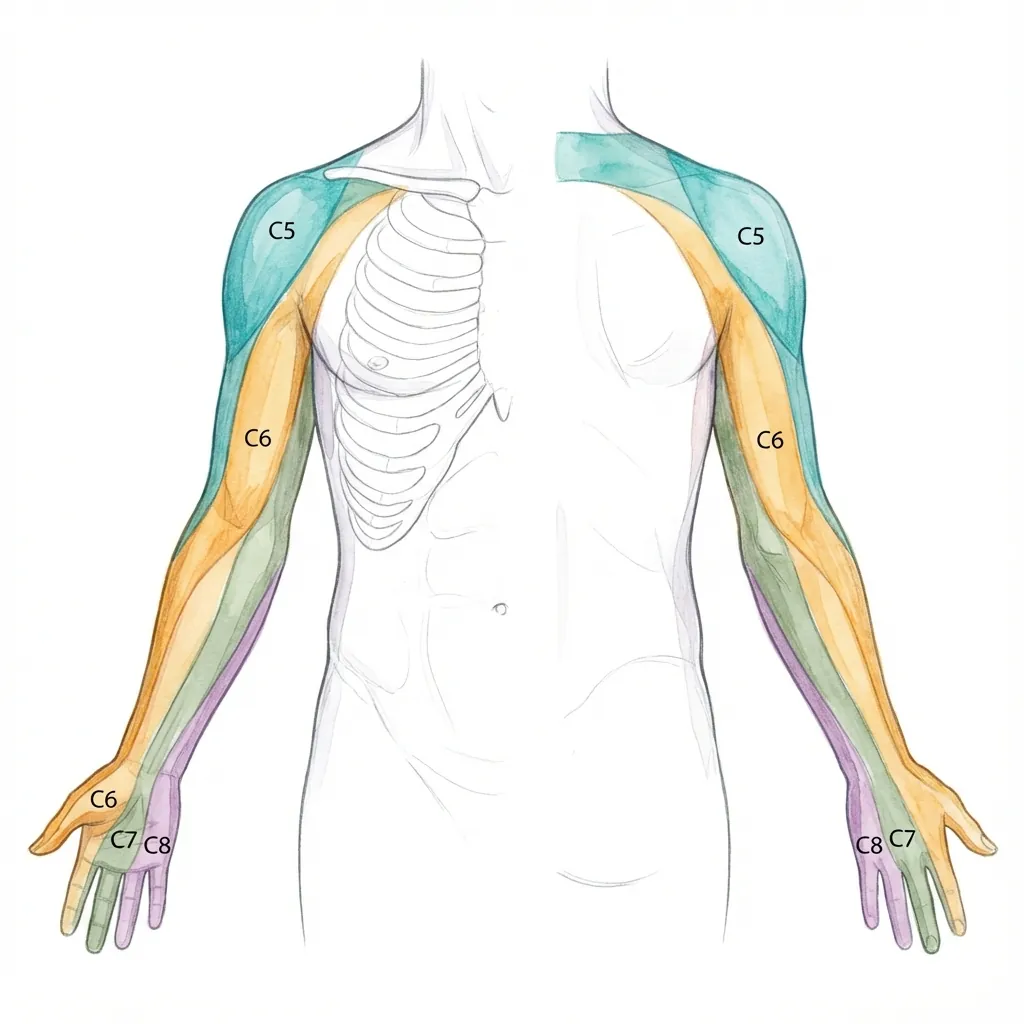
Each nerve root serves a specific skin region (dermatome) and muscle group
Radiculopathy Patterns
Caused by C5-C6 disc herniation
Forearm pain radiating to thumb and index finger
Thumb, index finger, lateral hand
Elbow flexion, wrist extension weakness
Diminished biceps reflex
Clinical Insight: When you describe your symptoms to a surgeon, the location pattern immediately suggests the level of pathology. Imaging (MRI) confirms it.
Radiculopathy
Pinched Nerve Root
Occurs when disc herniation or bone spurs compress the nerve root exiting the spine. Often affects one side only.
Prognosis: Often resolves without surgery (~90% of cases) with conservative treatment.
Myelopathy
Spinal Cord Compression
A much more serious condition where the main spinal cord itself is compressed. Can cause progressive, potentially irreversible neurological damage.
URGENT: Requires surgical evaluation within weeks to months. Prolonged compression causes irreversible damage.
Key Diagnostic Differences
| Feature | Radiculopathy | Myelopathy |
|---|---|---|
| Side Affected | Usually unilateral (one side) | Bilateral (both sides) |
| Primary Symptom | Arm pain in specific path | Gait/balance disturbance |
| Upper Limbs | Dermatomal numbness | Hand clumsiness |
| Lower Limbs | Usually unaffected | Stiffness, weakness |
| Urgency | Elective evaluation | Urgent surgical evaluation |
| Surgery Rate | ~10% require surgery | Most require surgery |
Surgical Planning & Imaging
How surgeons translate anatomy into surgical strategy—from imaging interpretation to precise implant selection.
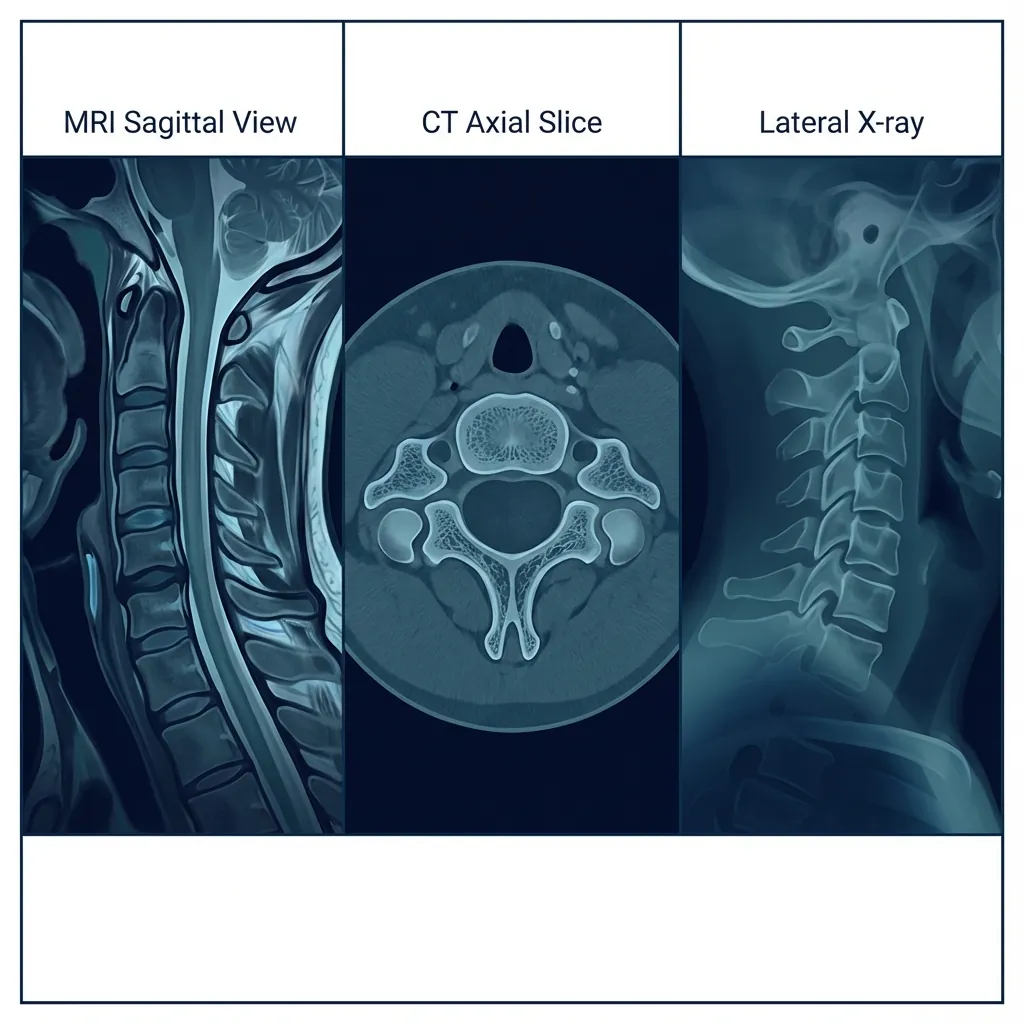
Magnetic Resonance Imaging
MRI
The gold standard for soft tissue evaluation. Uses magnetic fields and radio waves to create detailed images without radiation.
Strengths
- Excellent soft tissue detail (discs, cord, ligaments)
- Visualises cord signal changes (myelomalacia)
- No radiation exposure
- Can detect early disc degeneration
Limitations
- Static images only (no motion assessment)
- May exaggerate foraminal stenosis
- Contraindicated with some implants
- Longer scan time, claustrophobia issues
First-line for suspected disc herniation, cord compression, or radiculopathy
Pre-Operative Planning Checklist
A systematic approach ensures no critical factor is overlooked before surgical intervention.
Clinical Assessment
- Dermatomal pain pattern mapping
- Motor strength grading (0-5)
- Reflex assessment
- Myelopathy signs (Hoffmann, Babinski, gait)
Imaging Review
- MRI sagittal and axial sequences
- Disc level(s) correlating with symptoms
- Spinal cord signal changes
- Facet joint status at target level
Anatomical Measurements
- Disc height at affected level(s)
- Vertebral body dimensions
- Foraminal dimensions
- Cervical lordosis angle
Surgical Planning
- Implant size selection
- Approach planning (usually anterior)
- Adjacent segment evaluation
- Contraindication screening
Critical Measurements for Implant Selection
5-7mm
Determines implant height
15-18mm
Determines implant footprint
14-17mm
Determines AP dimension
20-40°
Guides angular selection
Anatomical Terminology
Medical language can be confusing. This glossary helps you decode the terms you'll encounter in reports, consultations, and research.
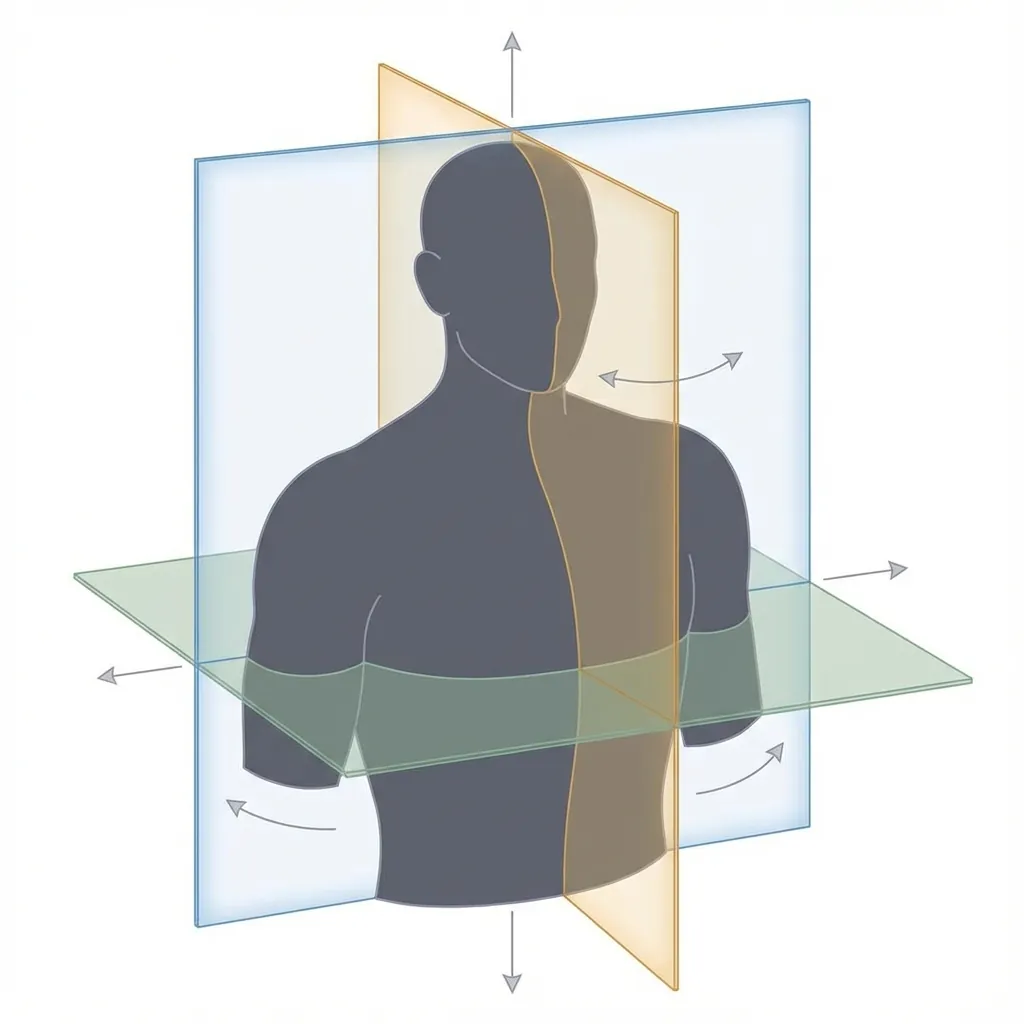
The three anatomical planes used in medical imaging
Anterior
Toward the front of the body
Example: The disc is anterior to the spinal cord
Posterior
Toward the back of the body
Example: The spinous process is the most posterior structure
Superior
Toward the head (above)
Example: C3 is superior to C4
Inferior
Toward the feet (below)
Example: C5 is inferior to C4
Lateral
Away from the midline (to the side)
Example: The foramen is lateral to the disc
Medial
Toward the midline (center)
Example: The spinal cord is medial to the nerve roots
Sagittal
Divides the body into left and right portions
Example: MRI sagittal view shows the spine from the side
Coronal
Divides the body into front and back portions
Example: Coronal view shows the body from the front
Transverse/Axial
Divides the body into upper and lower portions
Example: Axial MRI shows a cross-section through the disc
Flexion
Bending forward, decreasing the angle between segments
Example: Looking down involves cervical flexion
Extension
Bending backward, increasing the angle between segments
Example: Looking up involves cervical extension
Lateral Flexion
Side bending, tilting the head toward the shoulder
Example: Ear to shoulder movement
Rotation
Turning around the longitudinal axis
Example: Looking over your shoulder
Vertebral Body
The cylindrical, weight-bearing anterior portion of a vertebra
Pedicle
Short bony pillars connecting the vertebral body to the posterior elements
Lamina
Broad plates of bone forming the posterior wall of the spinal canal
Spinous Process
The posterior projection of a vertebra (the bumps you feel down your neck)
Foramen
An opening or passage (e.g., intervertebral foramen where nerves exit)
Facet Joint
Synovial joints between vertebrae that guide motion and share load
Stenosis
Narrowing of the spinal canal or foramina
Example: Central stenosis compresses the spinal cord
Herniation
Protrusion of disc material beyond its normal boundary
Example: Disc herniation can compress nerve roots
Radiculopathy
Disease or injury of a spinal nerve root causing radiating symptoms
Myelopathy
Disease or injury of the spinal cord itself
Spondylosis
Degenerative changes in the spine (general term)
Osteophyte
Bone spur—bony outgrowth at joint margins
Showing 25 of 25 terms
Directional Pairs
Movement Pairs
Common Suffixes
Bringing It All Together
The cervical spine is a remarkable feat of biological engineering. Understanding its anatomy is the foundation for informed decisions about spinal health.

Seven Vertebrae, Infinite Complexity
The cervical spine balances stability, mobility, and neural protection with remarkable precision.
Discs Are Engineering Marvels
The nucleus-annulus-endplate system provides load-bearing, shock absorption, and controlled motion.
Neural Architecture Is Vulnerable
The cord and nerve roots pass through narrow spaces susceptible to compression from degeneration.
Degeneration Follows a Cascade
Understanding the five-stage Kirkaldy-Willis cascade helps guide intervention timing.
Learning Objectives Complete
By reading this page, you should now understand:
The Big Picture
Your cervical spine is not just anatomy—it's the critical link between your brain and body. Every movement you make, every sensation you feel in your arms and hands, passes through these seven vertebrae.
When degeneration occurs, it's not random. It follows a predictable cascade that, when understood, becomes manageable. Early intervention preserves more function. Motion-preserving surgery, when appropriate, protects adjacent segments.
Understanding your anatomy empowers you to have informed conversations with your healthcare providers, ask the right questions, and make decisions that align with your long-term goals.
Explore Treatment Options
Learn about the differences between fusion and motion-preserving surgery.
Understanding Disc Arthroplasty
Deep dive into how artificial discs restore spinal function.
Candidacy Assessment
Find out if you may be a candidate for motion-preserving surgery.