
Hybrid Procedures
For complex multilevel spinal disease, a single surgical philosophy may not be optimal. Hybrid procedures combine motion preservation with strategic stabilisation—tailoring the approach to each individual spinal segment.
Motion Preserved
The Philosophy
60–75%
Hybrid procedures preserve 60-75% of motion compared to 20-40% with all-fusion approaches.
Risk Reduction
Adjacent-Segment Disease
50%
Significant reduction in adjacent-segment disease risk through strategic motion preservation.
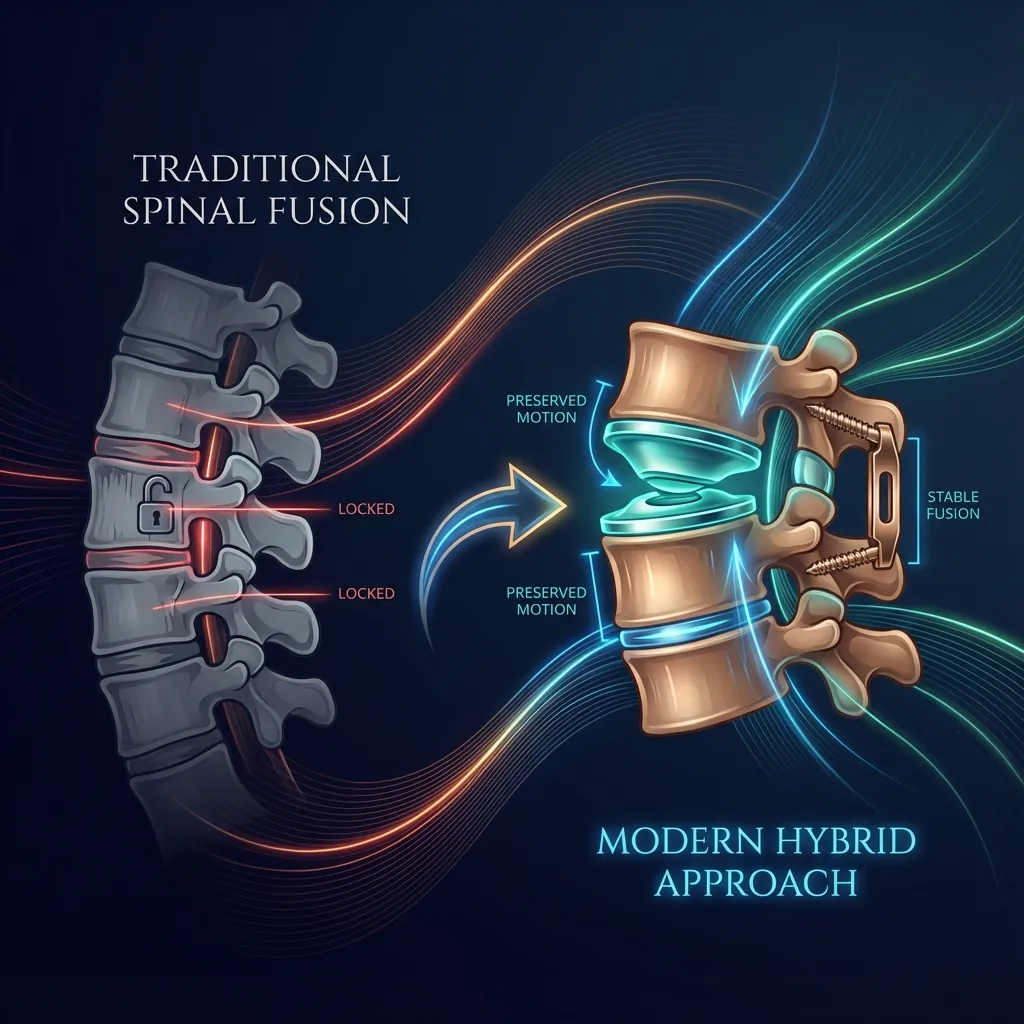
From Traditional Thinkingto Modern Hybrid Approaches
For decades, spine surgery followed a reductionist philosophy: identify all degenerative segments and treat them identically. This approach led to multilevel fusions—procedures that addressed multiple levels through rigid fixation.
The Problems with All-Fusion Philosophy
The Hybrid Philosophy
Hybrid surgery emerged from recognition of a simple truth: the spine is not homogeneous. Different segments often have different pathologies requiring different approaches.
Patient-Centric Outcomes
This tailored approach optimises both immediate pain relief and long-term functional outcomes, protecting the patient's spinal health across their remaining lifespan.
Why Hybrid ApproachesMake Biomechanical Sense
Multiple biomechanical and clinical investigations demonstrate that hybrid constructs create superior spinal mechanics compared to all-fusion approaches.

Key Biomechanical Advantages
Clinical Scenarios Favouring Hybrid
When degeneration is severe at some levels but preserved at others.
Three-level cervical case with severe C4–C5 and C6–C7 degeneration but excellent preservation at C5–C6. The well-preserved level is ideal for replacement; severely degenerated levels may require fusion.
When different levels have different primary pathologies requiring different treatments.
Lumbar case with discogenic pain and disc degeneration at L4–L5 (ideal for replacement) but severe facet arthropathy at L5–S1 (better suited for fusion).
When congenital stenosis or previous surgery at one level necessitates fusion, but adjacent levels have excellent disc quality.
Patient with prior fusion at one level now developing adjacent-level disease at a segment suitable for arthroplasty.
When functional outcomes are paramount and preserving mobility is a major priority.
Active 45-year-old requiring multilevel surgery. Preserving motion across as many segments as possible maximises long-term function.
When patients explicitly value maintaining normal spinal mobility over other considerations.
Patient-centred decision-making that prioritises motion preservation where anatomically appropriate.
Cervical HybridProcedures
Cervical hybrid procedures combine anterior cervical disc arthroplasty at one or more levels with anterior cervical discectomy and fusion (ACDF) at one or more levels within the same surgical intervention.

Two-Level Hybrid (Most Common)
- A/F: Arthroplasty at one level, fusion at adjacent level
- F/A: Fusion superior, arthroplasty inferior
Three-Level Hybrid
- A/F/F: Arthroplasty superior, fusions at inferior two levels
- A/A/F: Replacements at superior and middle, fusion at inferior
- F/A/F: Fusions at flanking levels, arthroplasty in middle
Skip-Level Hybrid
- Treating non-contiguous levels with different modalities
- Less common but sometimes appropriate
Placement pattern: Placing the replacement at the superior level preserves motion in the higher-mobility cervical region. Individual anatomy and specific pathology often dictate optimal configuration.
Lumbar HybridProcedures
Lumbar hybrid procedures combine anterior or anterolateral lumbar disc arthroplasty at one level with anterior lumbar interbody fusion (ALIF) at an adjacent level through coordinated approaches.
Two-Level Hybrid
Replacement at one level (typically L4–L5), fusion at another (typically L5–S1)
L4–L5 often selected for replacement (better bone quality, disc preservation); L5–S1 often selected for fusion (challenging anatomy, more severe facet disease)
Three-Level Hybrid
More complex configurations with multiple replacements and fusions
Strategic positioning based on pathology at each individual level
Biomechanical Advantagesof Hybrid Constructs
Understanding how hybrid constructs differ biomechanically from all-fusion approaches helps explain their clinical advantages.
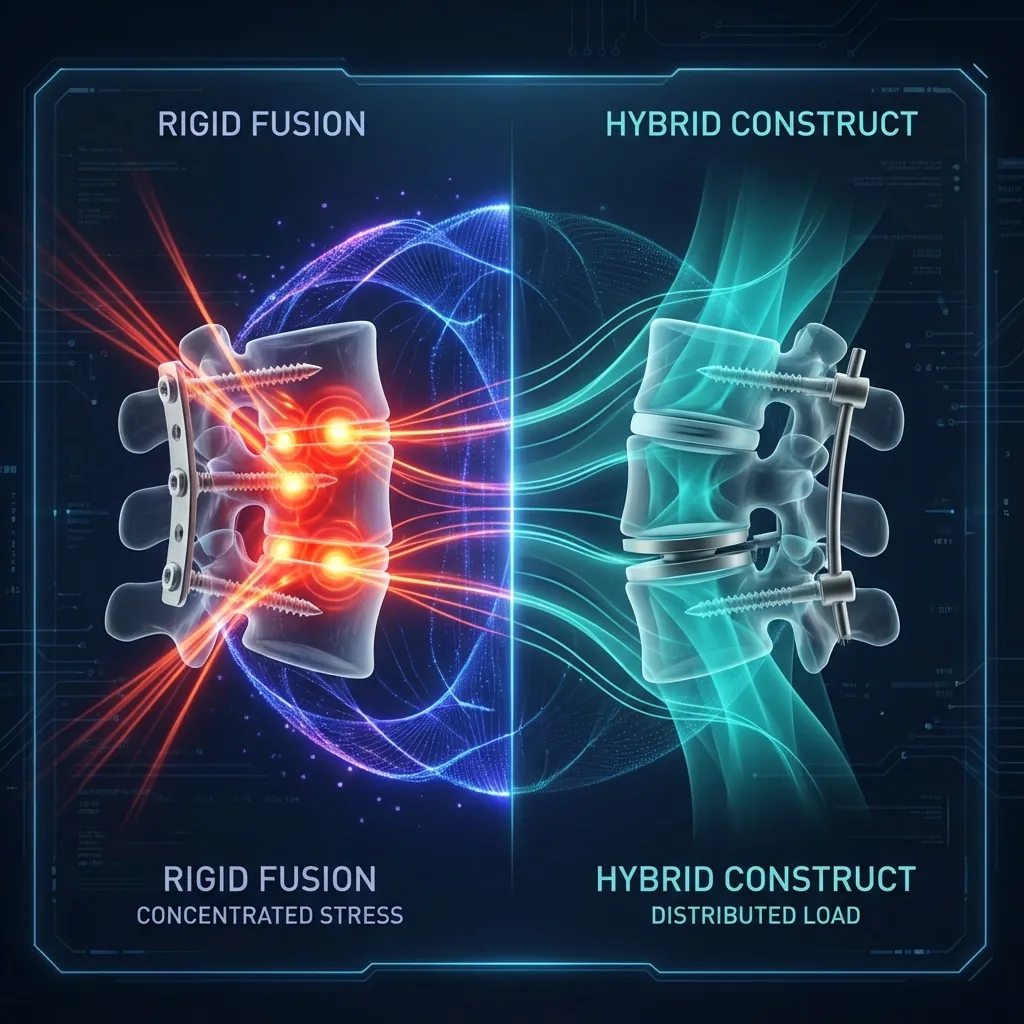
Load Distribution Patterns
Interpretation: Hybrid constructs dramatically reduce the biomechanical stress imposed on adjacent unfused segments—a key factor in preventing future adjacent-segment disease.
Range of Motion Preservation
Clinical Significance: Preserved mobility translates to better functional outcomes and reduced stiffness—particularly important for younger, more active patients.
The Mechanism of Adjacent-Segment Protection
The protective effect of hybrid constructs on adjacent segments operates through multiple mechanisms:
Reduced Compensatory Hypermobility
When fusion completely eliminates motion, adjacent segments must increase their motion by 50–100% above normal. Hybrid constructs prevent this excessive compensation.
More Physiological Loading Distribution
Motion-preserving levels allow loads to be distributed more naturally across spinal segments, rather than concentrating at rigid fusion interfaces.
Maintained Spinal Alignment
Hybrid constructs better maintain sagittal balance and spinal curvature compared to multilevel fusion, reducing kinematic stresses throughout the spine.
Progressive Advantage
The protective effect becomes increasingly apparent over time. At 10+ years, reduced adjacent-segment disease in hybrid cohorts becomes clinically evident.
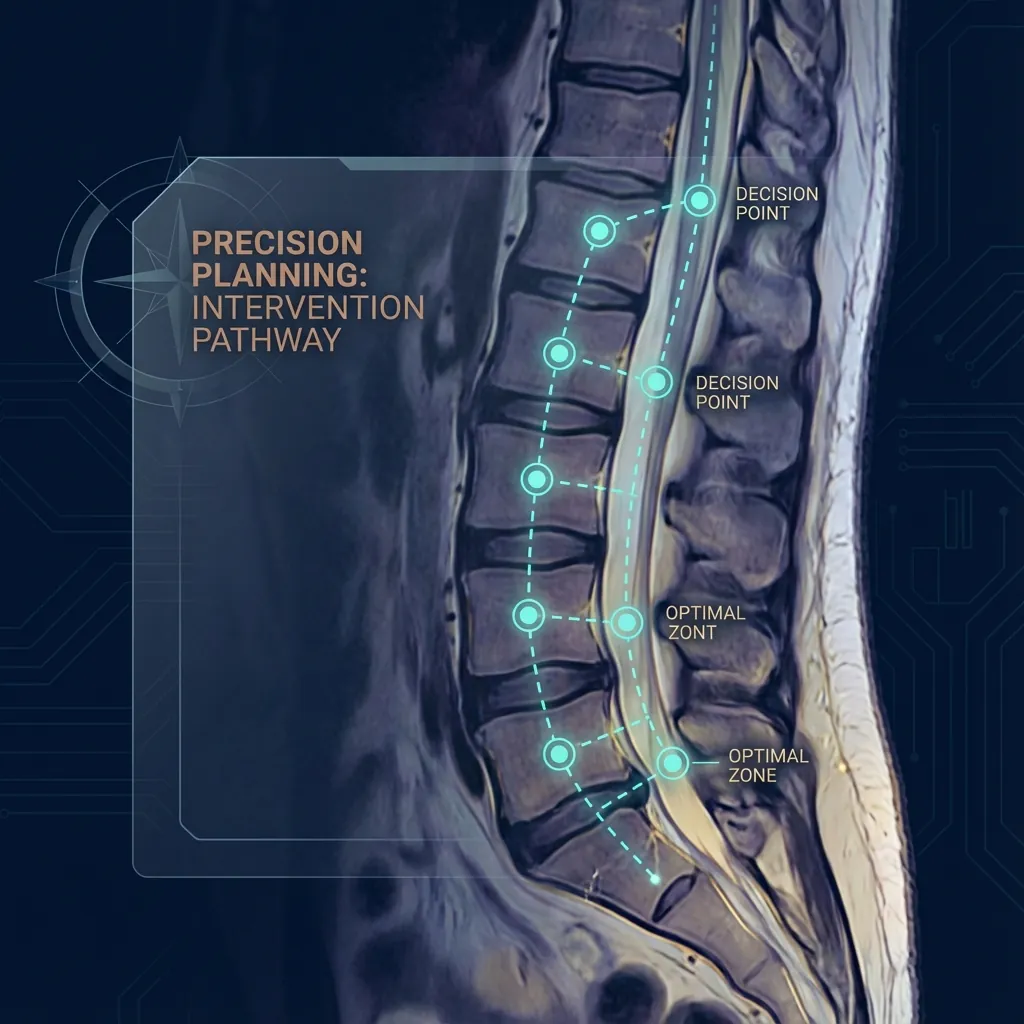
Assessment Frameworkfor Hybrid Procedure Planning
A systematic approach to determining the optimal hybrid configuration for each patient, considering imaging, individual level characteristics, and patient-specific factors.
Comparing Hybrid Procedureswith Alternatives
Understanding how hybrid procedures compare to all-fusion and all-motion-preserving approaches helps guide treatment decisions.

Hybrid vs All-Fusion Approaches
| Parameter | Hybrid Procedure | All-Fusion | Winner |
|---|---|---|---|
| Motion preservation | 60–75% | 20–40% | ✓ Hybrid |
| Adjacent-segment disease (10 yr) | 10–15% | 25–40% | ✓ Hybrid |
| Reoperation rate (10 yr) | 10–15% | 20–30% | ✓ Hybrid |
| Pain improvement | 50–60% | 50–60% | Tie |
| Functional improvement (ODI) | 45–60% | 45–55% | ✓ Hybrid |
| Operative time | Slightly longer | Baseline | ✓ Fusion |
| Operative complexity | Moderate-high | Moderate | ✓ Fusion |
| Return to work | Earlier (2–3 weeks) | Later | ✓ Hybrid |
| Long-term satisfaction | Maintained/improved | May decline with ASD | ✓ Hybrid |
| Quality of life | Better in active patients | Restricted mobility | ✓ Hybrid |
Hybrid vs Motion-Preserving Alone
Some patients are candidates for arthroplasty at all affected levels. The key distinction: Hybrid procedures are optimal when some but not all affected levels are suitable for replacement.
All levels suitable for replacement
One level unsuitable for replacement
Multiple levels unsuitable
Hybrid vs Staged Procedures
Some complex cases might be addressed through staged (sequential) procedures rather than single-stage hybrids. Most contemporary evidence favours single-stage hybrid procedures for appropriate candidates.
Single-Stage Hybrid
Single anaesthetic exposure
Single recovery period
Reduced total operative burden
Immediate biomechanical optimisation
Staged Approach
Allows assessment of initial intervention before proceeding
Potentially lower operative time per procedure
May be necessary if extensive decompression required
Clinical Outcomesand Long-Term Success
Long-term follow-up studies consistently demonstrate durable outcomes for appropriately selected hybrid procedure patients.

Cervical Hybrid
5–15 year follow-up data
- Clinical success rates85–92%
- Pain relief maintainedLong-term sustained
- Motion preservation at replacement levels75–85% of normal
- Adjacent-segment disease rates10–18%vs 25–35% in ACDF
- Reoperation rates (10-year)8–12%
- Patient satisfaction85–92%
Outcomes stable beyond 10 years: Available data extending to 12–15 years show no deterioration. No progressive stiffening of replacement levels observed.
Lumbar Hybrid
7–15 year follow-up data
- Pain relief (VAS back)50–65% reduction sustained
- Functional improvement (ODI)45–60% reduction sustained
- Reoperation rates13–16%vs 20–30% in fusion literature
- Work capacity return70–75% original employment
- Major complication rates3–5%
- Patient satisfaction80–90%
10+ year follow-up: No diminished outcomes in patients with very long follow-up. Sustained pain relief and durable functional improvement.
Predictors of Hybrid Procedure Success
Favourable Factors
Careful patient selection (appropriate indications)
Good preoperative pain-related disability (not too extensive)
Absence of major comorbidities
Good bone quality
Adequate disc height preservation
Appropriate surgical technique and implant selection
Less-Favourable Factors
Severe preoperative disability with multiple comorbidities
Osteoporosis
Extensive facet arthropathy
Revision surgery context
Even less-favourable cases often benefit from hybrid approaches, but outcomes are optimised with careful patient selection.
Complicationsand Safety
Hybrid procedures, when performed by experienced surgeons, demonstrate a favourable safety profile comparable to non-hybrid alternatives.

Transient Complications
Usually resolve without intervention
Temporary slowing of bowel function; managed with diet and medications; resolves within days to weeks
Normal postoperative response
Managed expectations important; not dangerous
Gradually improves
Potential Serious Complications
Rare but important to understand
Hybrid-Specific Considerations
- Hybrid procedures have comparable complication rates to non-hybrid alternatives
- The mixed nature of the construct (replacement + fusion) does not create additional complications
- Heterotopic ossification (bone formation around implants): More common with cervical arthroplasty; usually asymptomatic but occasionally limits motion
Risk Mitigation Strategies
Preoperative Optimisation
- Smoking cessation (substantially reduces all risk)
- Blood sugar optimisation in diabetics
- Cardiovascular optimisation
Intraoperative Technique
- Experienced vascular collaboration (lumbar procedures)
- Careful neural decompression
- Meticulous haemostasis
- Appropriate implant sizing and positioning
Postoperative Management
- Early mobilisation (reduces thromboembolic risk)
- Appropriate antibiotic coverage
- Pain management allowing activity progression
Realistic Expectationsand Decision-Making
Understanding what hybrid procedures can and cannot accomplish helps set appropriate expectations for your surgical journey.
What Hybrid Procedures WILL Accomplish
Pain relief: Typically 50–65% improvement in pain scores
Functional improvement: 45–60% improvement in disability indices
Neurological symptom relief: Radiculopathy symptoms typically improve substantially
Motion preservation: Significantly more spinal motion maintained vs all-fusion
Long-term durability: Outcomes sustained at 10–15 year follow-up
Reduced adjacent-segment disease risk: 50–60% reduction compared to all-fusion
What Hybrid Procedures WILL NOT Accomplish
Complete pain elimination: Most patients retain mild residual discomfort (1–2/10)
Immediate full recovery: Recovery takes months; return to full activities takes 3–6 months
Guaranteed prevention of future problems: ASD still occurs in 10–15% of patients
Perfect spinal function: Some patients experience residual limitations despite improvement
Realistic Recovery Timeline
Most patients report "substantial improvement" by 3 months and "return to normal" by 6 months, though final plateau may take 12 months.
Decision-Making Framework
Consider Hybrid When:
- Complex multilevel degenerative disease
- Some levels suitable for motion-preserving disc replacement
- Some levels require fusion for stability
- You value motion preservation and functional outcomes
- You seek lower risk of future adjacent-segment operations
- You've exhausted reasonable conservative care
- Symptoms significantly limit quality of life or cause progressive neurological deficit
Consider All-Fusion When:
- Multiple levels have severe degeneration with contraindications to replacement
- Extensive spinal deformity requires comprehensive stabilisation
- Significant instability (spondylolisthesis >4–5 mm) is present
Consider Motion-Preserving When:
- All symptomatic levels are suitable for disc replacement
- You strongly prioritise motion preservation
- You have single-level or carefully selected two-level disease
Next Steps in Your Evaluation
Gather Your Imaging
- MRI reports and images
- Flexion-extension X-rays if available
- Previous imaging for comparison
- CT imaging if available
Prepare Your History
- When did symptoms start?
- What treatments have you tried?
- Which activities aggravate symptoms?
- What functional goals do you have?
- What matters most to you in outcomes?
Schedule Consultation
- Bring imaging and medical records
- Discuss your specific anatomy and pathology
- Ask about your surgeon's experience with hybrid procedures
- Clarify your candidacy for hybrid vs other approaches
- Discuss realistic expectations for your individual case
Hybrid Proceduresat a Glance

When Hybrid Procedures Excel
Cervical Hybrid Advantages
vs ACDF
- 10.08° greater C2–C7 ROM postoperatively
- Reduced superior adjacent-segment motion
- Comparable pain/function outcomes
- Similar complication rates
- Less blood loss
Lumbar Hybrid Long-Term Data
7+ year follow-up
- 50.7%back pain improvement sustained
- 53.5%leg pain improvement sustained
- 45.9%functional improvement sustained
- 2.9%replacement-level reoperation rate
- 16.1%overall reoperation (vs 20–30% fusion)
Key Statistics: Hybrid vs All-Fusion
| Parameter | Hybrid Procedures | All-Fusion |
|---|---|---|
| Motion Preservation | 60–75% | 20–40% |
| Adjacent-Segment Disease (10 yr) | 10–15% | 25–40% |
| Reoperation Rate (10 yr) | 10–15% | 20–30% |
| Patient Satisfaction | 85–92% | 80–88% |
| Long-Term Durability | Stable at 15 years | May decline with ASD |
| Return to Work | Earlier | Later |
| Functional Quality of Life | Superior in active patients | Limited by stiffness |
Final Synthesis
Hybrid spine procedures represent a significant evolution in surgical philosophy—moving from rigid "one-size-fits-all" approaches to sophisticated, individualised, biomechanically optimised treatment strategies.
For appropriately selected patients with complex multilevel spinal pathology, hybrid procedures offer:
"Treat each spinal segment appropriately based on its specific pathological characteristics, preserving motion where possible whilst providing stability where necessary."
Remember
Hybrid procedures are a sophisticated, evidence-based approach to complex multilevel spinal disease. They are not suitable for every patient or every spinal condition, but for appropriately selected patients, they offer compelling advantages.
Your healthcare provider remains your most important resource for determining whether hybrid procedures are appropriate for your specific spinal condition, anatomy, pathology, and personal circumstances.
Engage in collaborative decision-making with an experienced spine surgeon, armed with the knowledge that hybrid procedures represent a thoughtful, biomechanically superior approach to managing complex multilevel spinal disease.