
Revision Arthroplasty
Revision surgery following spinal arthroplasty represents one of the most challenging scenarios in modern spine surgery. Unlike primary disc replacement procedures, revision surgery must address altered anatomy, previous implant-related changes, and complex biomechanical alterations.
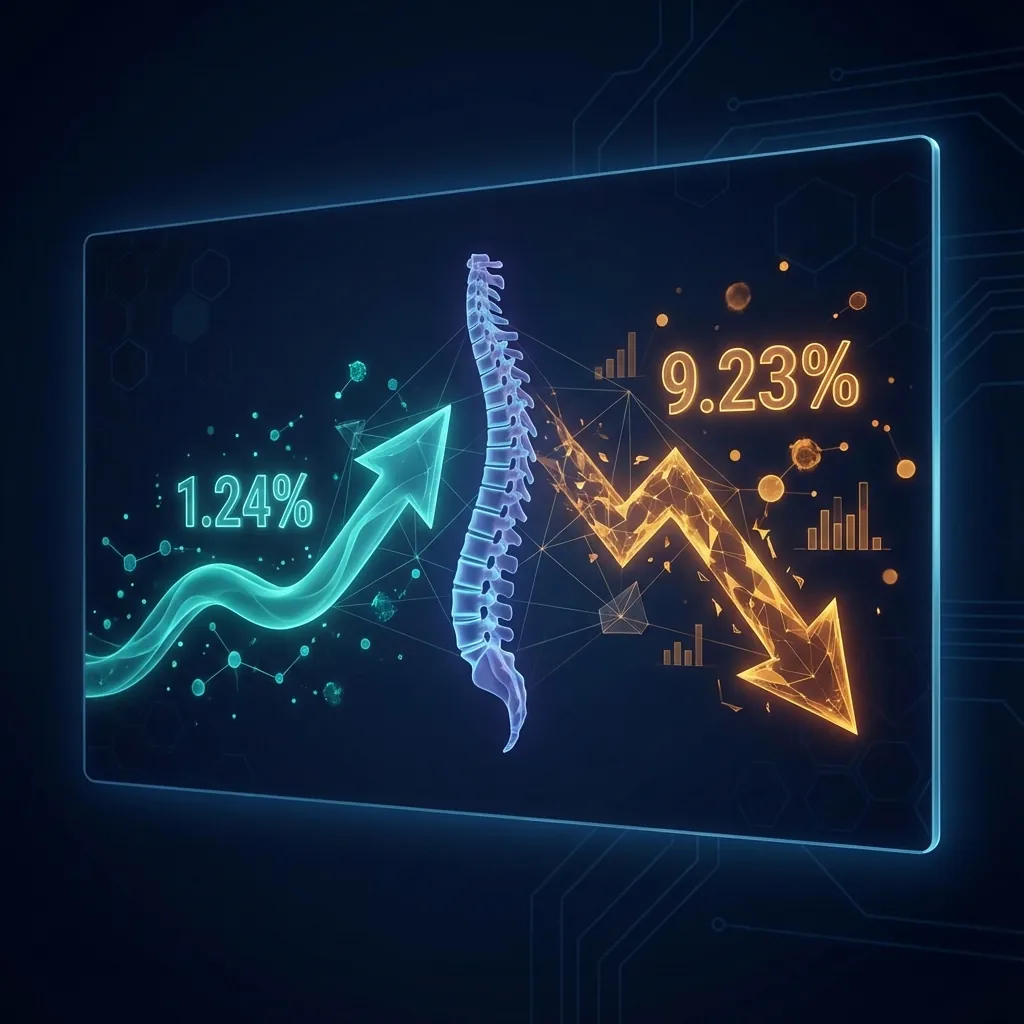
CDA 5-Year Revision Rate
1.24%
Compelling evidence of implant durability compared to 9.23% for ACDF.
Lower Risk vs Fusion
8.09x
Patients undergoing ACDF are 8.09 times more likely to require revision.
Revision Success Rate
80–86%
Patients reporting good to excellent outcomes following revision surgery.
Primary Arthroplasty Failure Rates
Understanding the incidence of disc arthroplasty failure provides important context. Recent large-scale studies provide reliable estimates demonstrating remarkably low revision rates.
Cervical Disc Arthroplasty
2024 Study (32,953 patients)
Key Finding: Primary disc arthroplasty revision rates are remarkably low—typically 0.7–3.9% at extended follow-up—demonstrating that modern prostheses are durable and mechanically reliable when properly selected and implanted.
Comparison to Fusion
Traditional fusion revision rates substantially exceed arthroplasty revision rates.
Lower Revision Risk
Patients undergoing ACDF are 8.09 times more likely to require revision compared to CDA patients.
Implant Durability
Modern prostheses engineered for decades of function with excellent biocompatibility.
Improved Selection
Refined patient selection criteria avoid high-risk candidates.
Technical Refinements
Optimised implant positioning and construct mechanics.
Learning Curve Completion
Surgeons now have substantial accumulated experience.
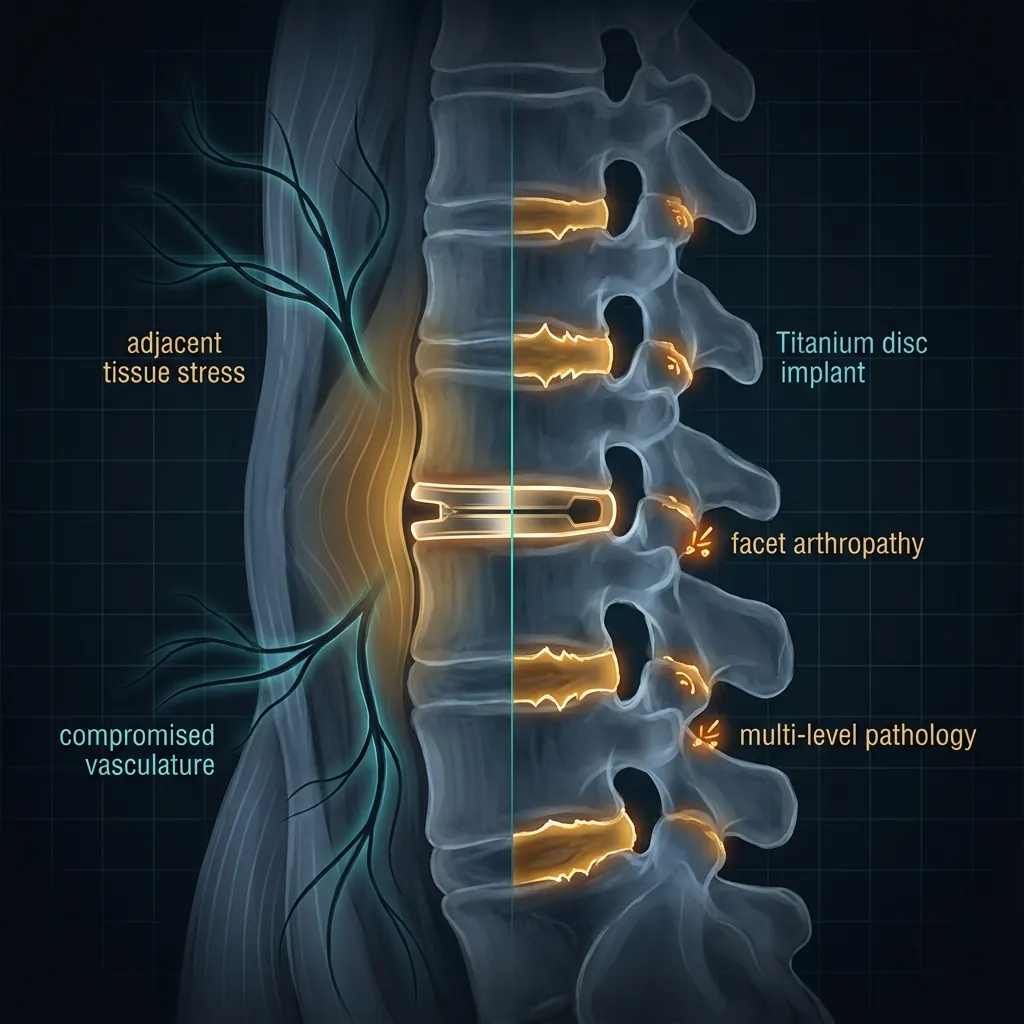
Mechanisms of Disc Arthroplasty Failure
Whilst revision rates remain low, understanding why failures occur is essential for guiding revision decision-making and preventing future revisions.
Pathophysiology
Surgical trauma providing inflammatory stimulus
Non-physiological motion patterns stimulating bone remodelling
Implant material and surgical trauma trigger localised inflammation
Biological predisposition: male sex, preoperative osteophytes
HO alone rarely necessitates revision surgery. Only when complete bony fusion causes clinical symptom deterioration might revision be considered.
Risk Factors for Revision After Arthroplasty
Certain patient factors and anatomical characteristics increase the risk of requiring revision surgery after primary arthroplasty.
Patient-Related
Age <50 Years
Higher revision rates due to longer life expectancy.
Male Sex
Associated with higher HO rates (Grade 3–4).
Osteoporosis
DEXA T-score <–2.5 increases subsidence/migration risk.
Obesity (BMI >30)
Higher HO rates and complication risk.
Smoking
Impairs healing and increases complication risk.
Diabetes
Affects bone healing and increases infection risk.
Anatomical
Severe Facet Degeneration
Grade 3–4 arthropathy substantially increases risk.
Severe Pre-existing Osteophytes
Extensive burden increases HO risk.
Inadequate Disc Height (<3mm)
Poor candidates for arthroplasty.
Cervical Kyphosis
Significant malalignment may require fusion.
Surgical
Implant Selection
Different devices carry different revision risks (e.g., M6-C).
Surgeon Experience
Learning curve effects evident in early experience.
Surgical Technique
Proper technique minimises complications.
Surgeon experience and proper technique minimise revision risk
Indications for Revision Surgery
Revision surgery is appropriately considered when patients with failed primary arthroplasty fail conservative management and require surgical intervention.
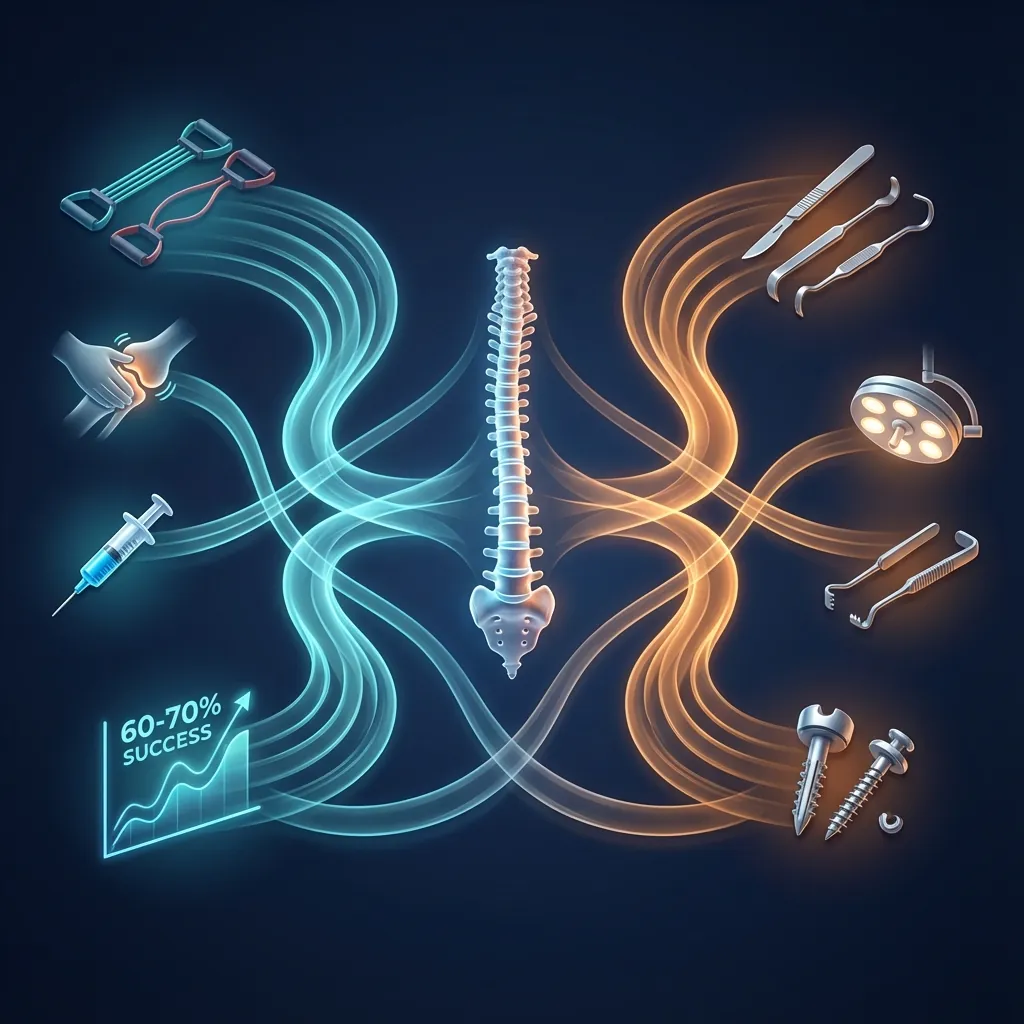
Systematic Approach
Before surgical revision, conservative treatment options must be exhausted. Approximately 60-70% of patients with symptomatic disc arthroplasty improve sufficiently with conservative care to avoid revision surgery.
Conservative Treatment First
60–70% improve sufficiently to avoid revisionMedical Management
Optimised anti-inflammatory medications
Analgesia as tolerated
Physical therapy targeting strengthening and stability
Interventional Procedures
Epidural steroid injections for radicular symptoms
Facet joint injections if facet-mediated pain suspected
Targeted nerve blocks for diagnostic clarification
Rehabilitation
Structured physiotherapy programmes
Postural training and ergonomics
Core stabilisation and neck/lumbar strengthening
Specific Indications for Revision
Persistent Radiculopathy/Myelopathy
Inadequate neural decompression
Implant subsidence causing re-stenosis
New adjacent-segment disease
Mechanical Complications
Implant migration or malposition
Severe subsidence requiring re-decompression
Complete HO with symptom deterioration
Failed Pain Management
Persistent discogenic pain at index level
Facet pathology unresponsive to interventions
Other
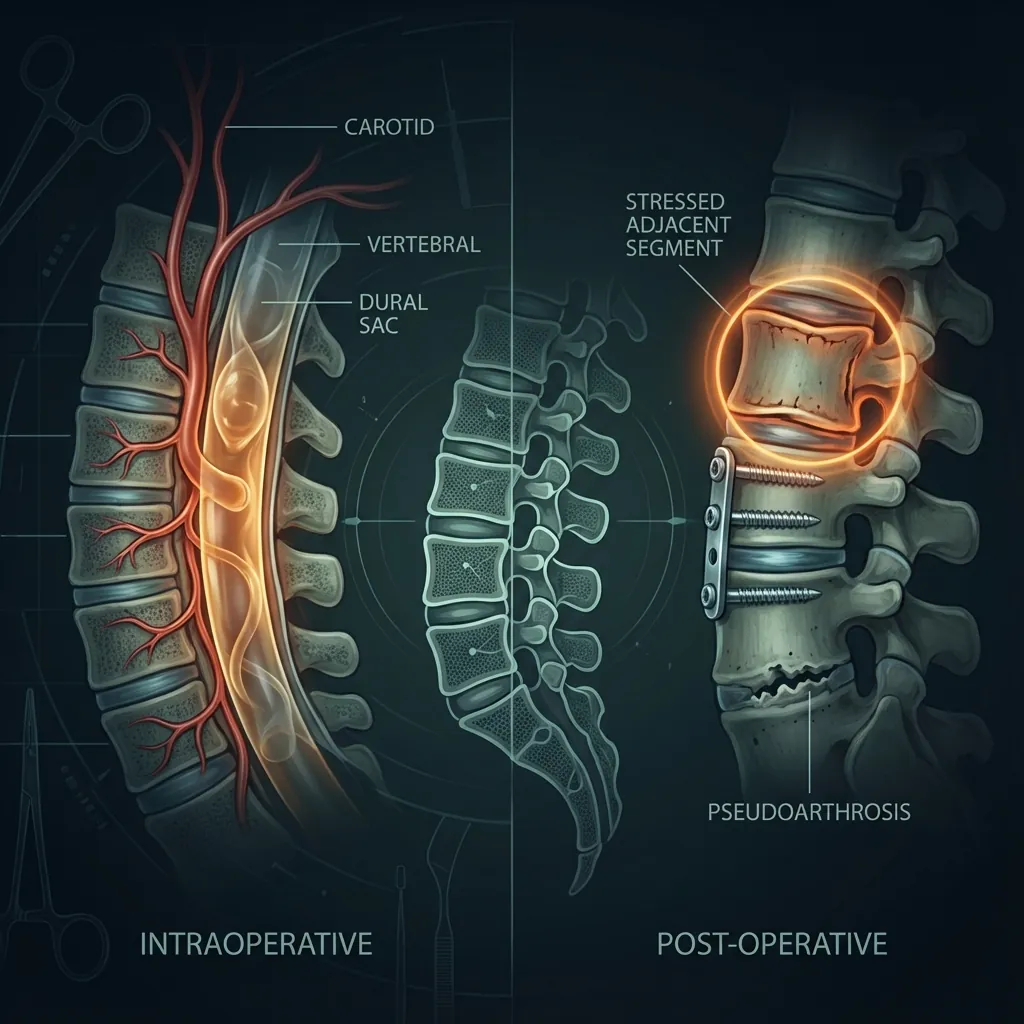
Pseudoarthrosis at fusion levels (hybrid)
Infection at operative site
Proven implant failure with symptoms
Adequate trial of conservative management (6–12 weeks minimum)
High-quality diagnostic imaging (MRI, flexion-extension X-rays)
Diagnostic injections to clarify pain source
Patient optimisation: smoking cessation, weight management
Timing Note: Revision surgery is typically not urgent unless neurological deterioration is evident. Most patients benefit from adequate conservative management before revision consideration.
Revision Surgical Strategies
When revision surgery becomes necessary, multiple approaches are available. The optimal strategy depends on specific failure mechanism, patient factors, and surgeon expertise.

Implant Removal with Anterior Fusion
Indications
Failed cervical arthroplasty in most scenarios
Persistent radiculopathy with inadequate decompression
Implant mechanical failure
Patient preference for fusion stability
Procedure
Reopening previous anterior cervical approach
Removing hardware and implant
Performing anterior cervical discectomy
Placing interbody cage with bone graft
Optional supplemental plate fixation
Outcomes
Advantages
Well-established technique
Provides immediate stability
Good long-term fusion rates
Predictable outcomes
Disadvantages
Eliminates motion at operative level
May accelerate adjacent-segment degeneration
Creates fusion scar tissue
Strategy Selection
Most revision cases (>70%) are best served by implant removal with fusion—a well-established technique with predictable outcomes.
Revision Surgery Outcomes
Understanding expected outcomes from revision arthroplasty failure helps guide patient counselling and expectations.
Operative Characteristics
Complications by Approach
Complication Overview
revision vs primary complication rate
Special Considerations in Revision Arthroplasty
Cervical and lumbar revision present unique challenges requiring tailored approaches.
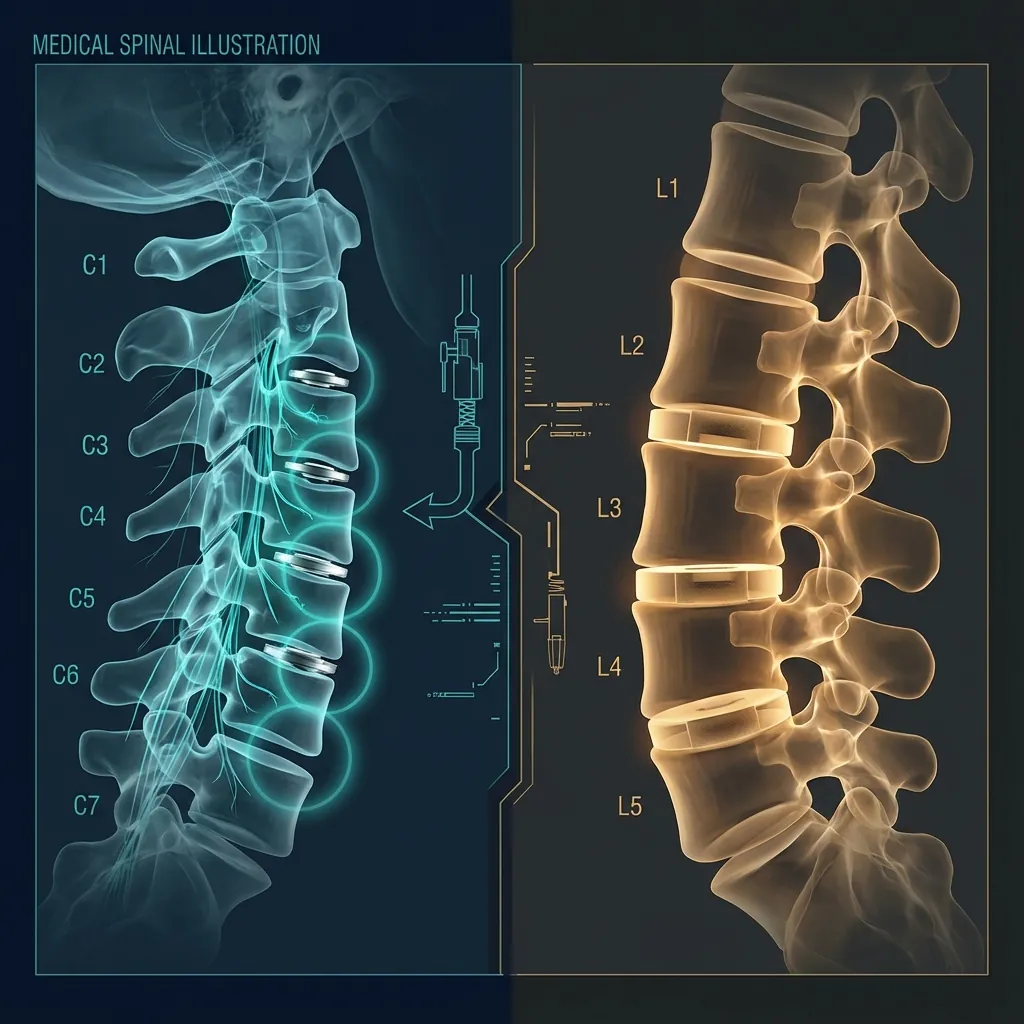
Cervical Revision Challenges
Previous approach creates scar tissue and distorted anatomy
Implant removal must avoid excessive bone loss
Bone stock issues require adequate cage sizing
Reoperation rate ~2.1% if approached anteriorly alone
Hybrid revision increasingly considered (fusion + adjacent arthroplasty)
Lumbar Revision Challenges
Anterior approach requires careful retroperitoneal navigation
Lumbar discs larger with more complex biomechanics
Removal must preserve vertebral body integrity
Hybrid options available for appropriate candidates
Very limited long-term revision data exist
Prior Fusion + New Arthroplasty
2025 Study (1,056 patients)
Patients with prior fusion developing symptomatic adjacent-segment disease may be candidates for arthroplasty at the new level (creating a hybrid construct).
Both approaches produce similar outcomes—previous fusion does not preclude successful arthroplasty at adjacent levels.
Complications of Revision Surgery
Understanding potential complications enables informed consent and proactive prevention strategies.
Intraoperative Complications
Vascular Injury
Risk slightly elevated due to distorted anatomy and scar tissue.
Neurological Injury
Risk comparable to primary with careful technique.
Excessive Bone Loss
Implant removal inevitably creates some endplate damage.
Inadequate Decompression
Persistent inadequate decompression represents technical failure.
Postoperative Complications
Infection
Rates slightly elevated in revision cases.
Pseudoarthrosis
Rates 1–5%, possibly slightly higher in revision.
Implant Malposition/Subsidence
Can occur if revision involves replacement.
Persistent Symptoms
Occurs in 10–20% of revision cases.
Anterior fusion revision approach has similar complication rates to primary surgery, whilst combined approaches have substantially elevated risk.
Decision Framework for Revision Arthroplasty
Selecting the appropriate revision strategy requires systematic evaluation of multiple clinical factors.
When to Consider Revision Surgery
Conservative care genuinely exhausted (6–12 weeks minimum)
Persistent or progressive neurological symptoms
Recurrent radiculopathy/myelopathy unresponsive to interventions
Documented implant mechanical failure
Intolerable pain unresponsive to conservative management
Strategy Selection by Factor
| Parameter | Fusion | Replacement | Hybrid |
|---|---|---|---|
| Failed implant salvageable | No | Yes | Depends on adjacent |
| Adequate bone stock | Not essential | Essential | Depends on approach |
| Patient age/longevity | Older patients | Younger patients | Middle-aged |
| Stability priority | Yes | No | Balanced |
| Surgeon experience | Fusion expertise | Arthroplasty expertise | Both required |
| Adjacent-segment disease | Not relevant | Not relevant | Yes—appropriate |
Individualised Strategy Selection
Different revision approaches suit different scenarios. The treating surgeon must carefully weigh patient-specific factors, including bone quality, overall health, and personal preferences, in conjunction with the specific failure mechanism identified.
The most common revision strategy—implant removal with anterior fusion—produces comparable complication rates to primary surgery and generally durable outcomes.
Key Principles of Revision Spinal Arthroplasty
When revision surgery becomes necessary, contemporary approaches produce generally favourable outcomes with careful patient selection and meticulous technique.
Primary Arthroplasty is Durable
True device failure rates remain exceptionally low (0.7–3.9% at 5+ year follow-up), demonstrating reliable function when appropriately selected and implanted.
Revision Reflects Exceptions
When revision becomes necessary, it usually reflects uncommon true device failure, poor initial patient selection, or technical error—not device inferiority.
Anterior Fusion Revision is Proven
The most common strategy—implant removal with anterior fusion—produces comparable complication rates to primary fusion and durable outcomes.
Strategy Selection is Individualised
Different revision approaches suit different scenarios. Implant removal with fusion remains most common, but replacement and hybrid increasingly have roles.
Outcomes are Generally Satisfactory
Approximately 80–86% of revision patients report good or excellent outcomes, with sustained pain improvement and functional restoration.
ASD Risk Continues
When revision involves fusion, subsequent adjacent-segment disease risk increases as expected, underscoring importance of careful surgical planning.
Remember
Revision spinal arthroplasty remains uncommon—a testament to the durability and clinical success of primary arthroplasty when appropriately performed and patient-selected. When revision becomes necessary, contemporary surgical strategies produce generally favourable outcomes with pain improvement, functional restoration, and durable results.
The key to optimal revision outcomes lies in careful patient evaluation, accurate diagnosis of specific failure mechanism, strategic revision approach selection, and meticulous surgical technique. Patients requiring revision surgery should engage in detailed discussions with experienced spine surgeons regarding specific options, expected outcomes, and realistic recovery expectations.