
Treatment Decisions Cervical And Lumbar Disc Replacement
A comprehensive guide providing evidence-based information to support informed decision-making through shared discussion with healthcare providers. The approach recognises that treatment decisions in spine surgery should be collaborative—incorporating clinical evidence, individual patient factors, realistic outcome expectations, and personal preferences.
Conservative Trial
Before Surgery
6-12 Weeks
Structured conservative treatment recommended before surgical consideration, unless progressive neurological deficit present.
ASD Reduction
With Motion Preservation
50-67%
Motion-preserving disc replacement reduces adjacent segment disease compared to fusion, particularly benefiting younger patients.
Decision Process
Patient-Centred Care
Collaborative
No single treatment is universally optimal. The most appropriate choice depends on individual circumstances, preferences, and long-term goals.
The Treatment Decision ProcessA Collaborative Approach
Patients presenting with symptomatic cervical or lumbar degenerative disc disease face a significant medical decision: whether surgical intervention is appropriate, and if so, which surgical approach best aligns with individual circumstances, preferences, and long-term goals.
No single treatment is universally optimal; rather, the most appropriate choice depends on multiple interconnected factors that must be carefully considered together.
Key Decision Factors

Disease Characteristics
The anatomical and pathological features of your spinal condition guide treatment selection.
This framework emphasises that treatment decisions in spine surgery should be collaborative—incorporating clinical evidence, individual patient factors, realistic outcome expectations, and personal preferences.
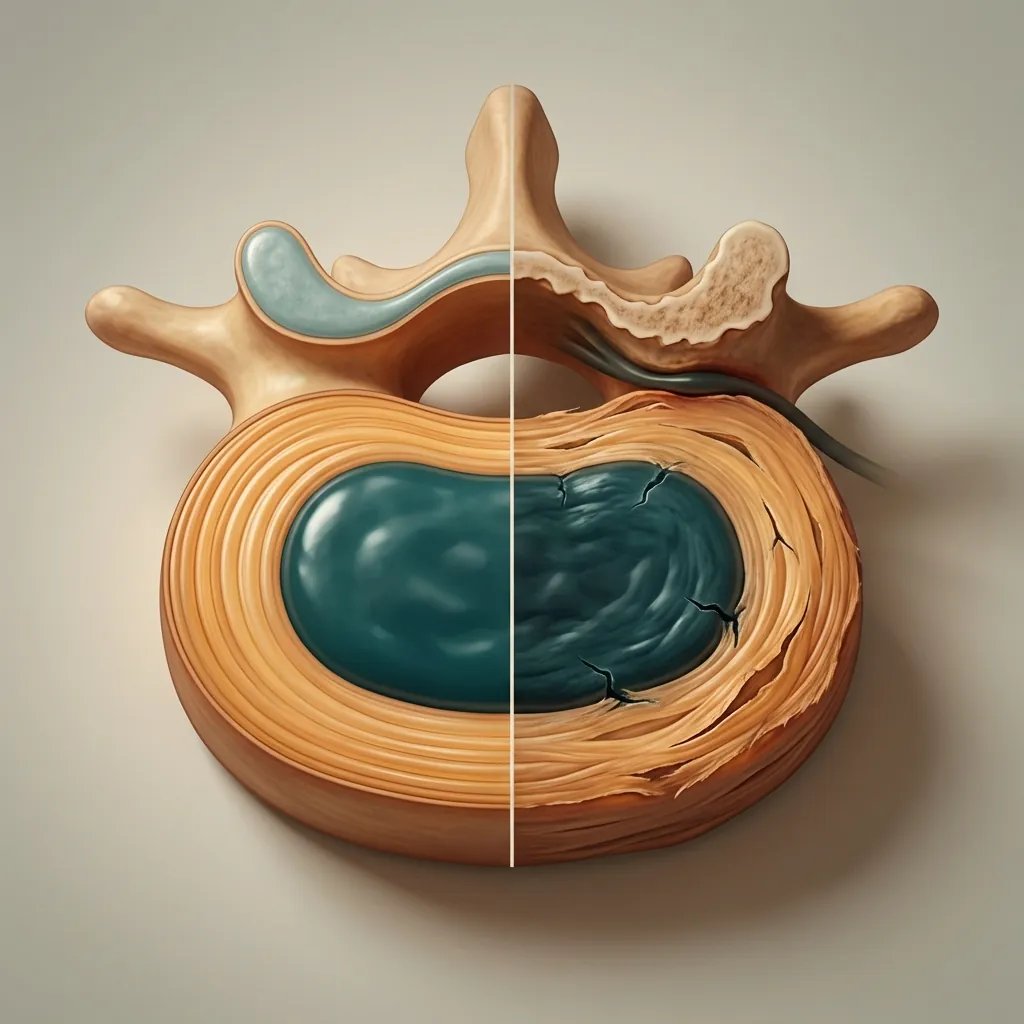
Understanding Spinal Degenerative Disc DiseaseWhen Discs Become Symptomatic
Degenerative disc disease (DDD) represents the natural ageing process of spinal discs—the shock-absorbing structures between vertebrae. Over time, discs lose hydration, develop small tears, and may bulge or herniate, potentially compressing nerve roots (radiculopathy) or spinal cord (myelopathy).
Important: This process affects an estimated 80–90% of adults by age 60, though not all develop symptomatic disease. Degenerative changes on imaging do not automatically indicate the need for treatment.
Symptomatic Presentations
Radiculopathy
Nerve Root Compression
Sharp, burning pain radiating into arm (cervical) or leg (lumbar); often accompanied by numbness, tingling, or weakness in specific distributions.
Natural History
Without Surgery
The natural history of degenerative disc disease is heterogeneous. Approximately 50–70% of patients with radiculopathy experience spontaneous improvement over weeks to months through natural inflammatory resolution and resorption of disc herniations.
However, some patients experience persistent or progressive symptoms affecting work capacity, functional independence, and quality of life.
Important Exception
Cervical Myelopathy
Cervical myelopathy represents an exception to the general pattern: untreated myelopathy often progresses, potentially resulting in permanent neurological deterioration.
Early surgical intervention is generally recommended when clear evidence of myelopathy exists.
Conservative & Interventional ManagementEvidence-Based First-Line Care
For most patients with symptomatic degenerative disc disease (excluding progressive myelopathy), initial conservative management is appropriate. Evidence-based approaches combine multiple treatment modalities for optimal outcomes.
Patients achieve symptom resolution without surgery
Recommended conservative trial before surgical consideration
Typical duration of injection benefits
Treatment Approaches

Physical Therapy & Rehabilitation
Structured programmes addressing postural dysfunction, core stabilisation weakness, and movement patterns.
Key Components
Evidence
Research demonstrates that early, progressive physical therapy significantly improves outcomes in radiculopathy patients, with 50–70% achieving symptom resolution without surgery.
Timeline for Conservative Management
Most clinical guidelines recommend 6–12 weeks of structured conservative treatment before considering surgical intervention, assuming the patient is not experiencing progressive neurological deficit. This timeframe permits assessment of natural symptom improvement and establishes whether conservative measures provide adequate relief.
Exception: Some patients experience intolerable symptoms or functional impairment despite conservative efforts, or develop concerning neurological findings suggesting progression. In these cases, earlier surgical consideration becomes appropriate.
Surgical Candidates & Selection CriteriaWho Benefits from Surgery?
Not all patients with degenerative disc disease are appropriate surgical candidates. Selection should consider multiple factors to ensure optimal outcomes and appropriate resource utilisation.
Selection Framework

Clinical Presentation Alignment
Symptoms must correlate with imaging findings.
Age Considerations
Age per se is not a contraindication to disc replacement. The motion-preserving advantages may be particularly beneficial for younger patients (typically <65 years) who will live decades beyond surgery and experience cumulative effects of spinal biomechanics. Older patients (>75 years) may also be excellent candidates if medically stable and appropriately selected.
Patient age influences the relative importance of motion preservation. A younger patient with 50 years of remaining life expectancy may experience greater long-term benefit from motion preservation compared to an elderly patient; conversely, advanced age alone does not preclude excellent surgical outcomes.
Progressive myelopathy with neurological deficit
Requires urgent surgery but may have different implications for procedure selection.
Severe osteoporosis with compromised bone quality
May limit disc replacement candidacy; fusion may be preferable.
Severe facet joint arthritis (grade 3–4)
May be better managed with fusion than arthroplasty.
Moderate-to-severe endplate damage
May compromise osseointegration and implant stability with arthroplasty.
Prior spinal fusion at operated level
Generally precludes arthroplasty; extension fusion or hybrid approaches considered.
Severe smoking or non-compliance
Poor bone healing and higher complication rates.
Preoperative Medical Evaluation
Comprehensive preoperative evaluation should address the following areas to ensure optimal surgical outcomes:
Surgical Treatment Options OverviewThe Treatment Spectrum
Surgical options for symptomatic cervical and lumbar degenerative disc disease exist on a spectrum from motion-preserving arthroplasty to fusion approaches. The choice between these options represents one of the most significant decisions in the treatment pathway.
Motion-Preserving
Disc Replacement
Maintain segmental motion at the operated level through implantation of artificial discs. This preserves physiological spinal biomechanics and reduces mechanical stress on adjacent segments.
Advantages
Considerations
Each approach offers distinct advantages and disadvantages requiring detailed discussion with surgical providers. The optimal choice depends on individual patient factors, pathology characteristics, and long-term goals.
Cervical Disc Replacement vs ACDFEvidence-Based Comparison
Multiple randomised controlled trials and meta-analyses compare cervical disc replacement to ACDF. Here we present the comprehensive evidence to support your treatment decision.
Cervical Disc Replacement (CDR)
Motion-Preserving
Key Metric
Anterior Cervical Discectomy & Fusion (ACDF)
Fusion
Key Metric
Key Differentiator
One landmark 10-year study reported composite clinical success of 62.4% for CDR versus 22.2% for ACDF (P<0.0001), representing a dramatic long-term advantage for arthroplasty.
Choosing Between CDR and ACDF
| Factor | CDR | ACDF |
|---|---|---|
| Patient age & life expectancy | Stronger benefit for younger patients (<65) | Similar outcomes in older patients |
| Symptom type | Excellent for radicular symptoms | Excellent for radicular symptoms |
| Imaging characteristics | Preserved facet joints favour CDR | Severe facet arthritis may favour ACDF |
| Occupational demands | Full activity resumption | Full activity resumption |
| Motion preservation preference | Maintains spinal motion | Eliminates segmental motion |
| Surgeon expertise | Requires specific training | Well-established techniques |
Lumbar Disc Replacement vs FusionLong-Term Outcome Comparison
Randomised controlled trials and meta-analyses comparing lumbar total disc replacement to fusion demonstrate important differences, particularly in long-term outcomes and adjacent segment preservation.
Lumbar Total Disc Replacement (TDR)
Motion-Preserving
Key Metric
Lumbar Fusion (ALIF, PLIF, TLIF)
Fusion
Key Metric
Key Differentiator
At 5-year follow-up, TDR demonstrates significantly lower reoperation rates compared to fusion, primarily driven by lower adjacent segment disease requiring reoperation.

Perioperative Considerations
Both procedures carry risks of vascular injury, visceral injury, and infection (all <2%). Lumbar disc replacement requires careful dissection of retroperitoneal structures.
Important: Experienced vascular and general surgical support during TDR is important for optimal safety outcomes.
Gastrointestinal Function
Both procedures carry ileus risk (temporary intestinal paralysis). Early mobilisation significantly reduces this risk.
Lumbar procedures carry slightly higher initial ileus risk due to retroperitoneal dissection, but this typically resolves within 24-48 hours.
Clinical Scenarios & Decision FrameworkReal-World Applications
Explore how treatment decisions are made in different clinical scenarios. Each case illustrates the application of evidence-based decision frameworks to individual patient circumstances.
Patient Scenarios
Young Patient with Single-Level Radiculopathy
Age 35
Clinical Presentation
6 weeks of progressive arm pain, numbness, and mild weakness; imaging confirms disc herniation compressing nerve root at single level; failed 6 weeks of physical therapy and injections.
Relevant Considerations
Decision Framework
For this patient, cervical disc replacement offers substantial long-term advantages. The 50-year lifespan ahead creates significant potential for adjacent segment degeneration with fusion (occurring in 12–18% by 10+ years). Motion-preserving disc replacement reduces this risk to approximately 6%. This difference is clinically and prognostically significant.
Expected Outcomes with CDR
Expected Outcomes with ACDF
Recommended Approach
Cervical disc replacement represents the better long-term choice for this patient, assuming imaging is appropriate and no contraindications exist.

The Shared Decision-Making ProcessPartnership in Treatment Decisions
Research on shared decision-making in spine surgery demonstrates that effective patient-provider communication improves satisfaction, reduces complications, and optimises outcomes. Here we outline the ideal shared decision-making process.
Elements of Effective SDM

Comprehensive Patient Education
The provider discusses disease natural history, treatment alternatives, expected outcomes, realistic recovery timelines, and risks of each approach.
Time constraints
Thorough shared decision-making requires time; busy clinics may not permit adequate discussion.
Request additional consultation time or pre-visit materials
Surgeon advocacy bias
Surgeons may unconsciously advocate for approaches they perform frequently rather than presenting balanced alternatives.
Ask about all treatment options regardless of surgeon preference
Patient factors
Patients may defer to surgeon authority rather than engaging in true shared decision-making.
Prepare questions in advance and advocate for your preferences
Communication skills
Not all surgeons receive training in shared decision-making communication techniques.
Bring this guide or similar resources to facilitate discussion
Information overload
Excessive technical detail may overwhelm rather than inform patients.
Ask for summaries and written information to review later
Effective Patient Questions for Surgeons
Patients should feel empowered to ask these questions during surgical consultations:
"What is your experience with each approach, and what are your complication rates?"
Surgeons should be transparent about experience and outcomes
"What are the short-term and long-term differences between these options?"
Understanding recovery trajectory and long-term implications is essential
"Which approach do you recommend for my specific situation, and why?"
The surgeon's recommendation, with reasoning, provides valuable perspective
"What will happen if surgery doesn't relieve my symptoms?"
Realistic discussion of revision options and persistent symptom management
"How will my daily life be different after surgery—work, activities, limitations?"
Functional outcomes and activity restrictions are critical concerns
"What are the risks specific to my medical situation?"
Individual comorbidities may modify risk profiles
"How do I prepare for surgery, and what should I expect during recovery?"
Understanding the process reduces anxiety and improves compliance
Special Populations & ConsiderationsIndividualised Management
Certain patient populations require additional consideration and preoperative optimisation. Understanding these factors helps ensure the best possible surgical outcomes.

Significant Medical Comorbidities
Diabetes, Cardiac, Pulmonary, Renal
Patients with diabetes, cardiac disease, pulmonary disease, or renal dysfunction may face higher operative risk. These patients require preoperative optimisation.
Management Approach
Both disc replacement and fusion carry comparable risk profiles in medically complex patients. However, disc replacement's potentially longer operative time may be relevant in high-risk individuals.
Important Note
Each patient's individual circumstances require personalised assessment. The considerations above provide general guidance, but your surgical team will develop a tailored plan based on your specific health profile and goals.
Long-Term Responsibilities & ExpectationsRealistic Recovery Timeline
Patients should understand the recovery trajectory and their role in achieving optimal long-term outcomes. Successful results require sustained engagement in rehabilitation and healthy lifestyle practices.
Recovery Timeline

Initial Recovery
Weeks 0-2
Pain management, protected mobilisation, wound healing. Most patients experience significant comfort improvement.
Key Milestones
Long-Term Activity Maintenance
Successful long-term outcomes require sustained engagement in healthy lifestyle practices:
Regular Physical Activity
Patients who maintain aerobic fitness and core strengthening experience better long-term outcomes than those becoming sedentary.
Proper Ergonomics
Workplace and home environment optimisation reduces recurrent pain risk.
Weight Management
Maintaining healthy weight reduces spinal loading and long-term degenerative stress.
Smoking Cessation
For smokers, continued abstinence improves long-term outcomes.
Regular Follow-Up
Patients should maintain scheduled follow-up appointments and imaging surveillance as recommended by their surgeon.
Cost & Healthcare Access in AustraliaUnderstanding Your Options
Australia's healthcare system provides multiple pathways to access spinal surgery. Understanding these options helps you make informed decisions about your care.

Medicare Benefits Schedule
Government Rebates
In Australia, both cervical and lumbar disc replacement and fusion procedures are eligible for Medicare Benefits Schedule (MBS) support, reflecting their evidence-based status as appropriate treatments for symptomatic degenerative disc disease.
Key Features
Considerations
Cost-Effectiveness Comparison
Cervical Disc Replacement
Evidence suggests CDR represents good value for money compared to ACDF, considering superior long-term outcomes and similar initial costs.
The reduction in adjacent segment disease requiring reoperation represents substantial long-term savings.
Lumbar Disc Replacement
Lumbar TDR demonstrates cost-effectiveness compared to fusion, particularly when accounting for lower revision rates.
Better return-to-work outcomes provide additional economic benefit for working patients.
Conclusion & Decision-Making SummaryKey Principles for Treatment Decisions
Several evidence-based principles should guide decisions regarding cervical and lumbar disc replacement versus fusion. Here we summarise the key considerations and provide actionable next steps.
Key Principles
Motion preservation matters for long-term outcomes
Extensive evidence demonstrates reduced adjacent segment disease with motion-preserving approaches, particularly important for younger patients with longer life expectancies.
Short-term outcomes are comparable
Pain relief, disability improvement, and return to work timelines are essentially equivalent between disc replacement and fusion. The differentiation occurs at longer follow-up (5–10+ years).
Patient age and life expectancy are important considerations
Younger patients derive greater benefit from motion preservation; older patients with limited life expectancy may achieve equivalent functional outcomes with either approach.
Individual disease characteristics matter
Imaging characteristics (facet arthritis, endplate damage, disc height), symptom type (radicular vs. axial), and number of affected levels guide approach selection.
Shared decision-making optimises outcomes
Patient preferences, occupational demands, medical comorbidities, and values should guide final decisions in partnership with surgical providers.
Both approaches are evidence-based
Neither disc replacement nor fusion is universally superior; the optimal choice depends on individual circumstances, and patients should feel confident in either appropriately selected approach.
Final Recommendations
Younger patients (<65 years) with single or two-level disease
Cervical disc replacement or lumbar total disc replacement should be strongly considered, given substantial long-term advantages regarding motion preservation and adjacent segment disease reduction.
Older patients (>75 years) with excellent medical status
Either approach is appropriate; patient preference and specific imaging characteristics should guide selection.
Patients with contraindications to arthroplasty
Fusion represents excellent treatment providing reliable long-term relief despite motion elimination.
Patients with uncertain preferences
Detailed discussion with surgeons should clarify individual values, clarify realistic expectations, and permit informed collaborative decisions.
Making Your Decision
Patients should discuss individual recommendations with their treating surgeons, who can provide personalised guidance based on detailed clinical assessment and imaging review.
Moving Forward: Your Next Steps
Ensure adequate conservative management
Most respond favourably to 6–12 weeks of structured physical therapy, NSAIDs, and activity modification.
Seek second opinions if desired
Consultation with different surgeons may provide additional perspectives.
Engage in thorough shared decision-making
Ensure complete understanding before committing to elective surgery.
Prepare comprehensively
Optimise medical comorbidities, cease smoking, and discuss preoperative expectations.
Commit to postoperative rehabilitation
Active engagement in therapy and home exercises optimises outcomes.
Maintain long-term lifestyle modifications
Regular activity, proper ergonomics, and weight management preserve benefits.
Patients should discuss individual recommendations with their treating surgeons, who can provide personalised guidance based on detailed clinical assessment and imaging review.