
Lumbar Disc Replacement Motion-Preserving Surgery
A fundamentally different strategy to treating degenerative disc disease. Rather than rigidly fusing the spine, modern artificial lumbar disc implants replace the degenerated disc whilst preserving your lower back's natural motion and biomechanics.
Years Research
Clinical Evidence
25+
Comprehensive long-term outcome studies spanning 7–21 years establish lumbar arthroplasty as safe, effective, and superior to fusion for appropriately selected patients.
ASD Reduction
Adjacent Protection
50-67%
Arthroplasty reduces adjacent-segment disease rates to 10–15% at 10 years compared to 30–45% with fusion—potentially preventing future operations.
Satisfaction
Long-Term Success
80-90%
Patient satisfaction rates of 80–90% sustained at 10–15+ years follow-up with no evidence of progressive deterioration over time.
A FundamentallyDifferent Strategy
Lumbar degenerative disc disease is one of the most common causes of chronic lower back pain, leg pain, and disability in working-age adults. For decades, the standard surgical approach has been anterior lumbar interbody fusion (ALIF) or posterolateral fusion—procedures that remove the diseased disc and permanently fuse the vertebrae together.
These approaches effectively address acute pain and neurological symptoms but come with significant long-term consequences: loss of motion at the fused level, accelerated degeneration of adjacent segments, and higher reoperation rates over time.
Lumbar Disc Arthroplasty Represents a Fundamentally Different Strategy
Rather than rigidly fusing the spine, modern artificial lumbar disc implants replace the degenerated disc whilst preserving your lower back's natural motion and biomechanics.
Comprehensive long-term outcome studies spanning 7–21 years have established that lumbar arthroplasty is safe, effective, and superior to fusion for appropriately selected patients.
Understanding Lumbar DiscDegeneration
Your lumbar spine (lower back) is a remarkable structure consisting of five vertebrae (L1–L5) separated by six intervertebral discs. The lowest two lumbar discs—L4–L5 and particularly L5–S1—bear the greatest loads and are most prone to degeneration.

Nucleus Pulposus
The inner gel-like centre providing shock absorption and load transmission
Annulus Fibrosus
The outer fibrous material containing the nucleus and providing structural integrity
Vertebral Endplates
The cartilaginous interfaces between disc and bone, distributing loads evenly
Nerve Supply
The outer disc is richly innervated with pain receptors, whilst the inner nucleus is relatively insensitive
The Degeneration Process
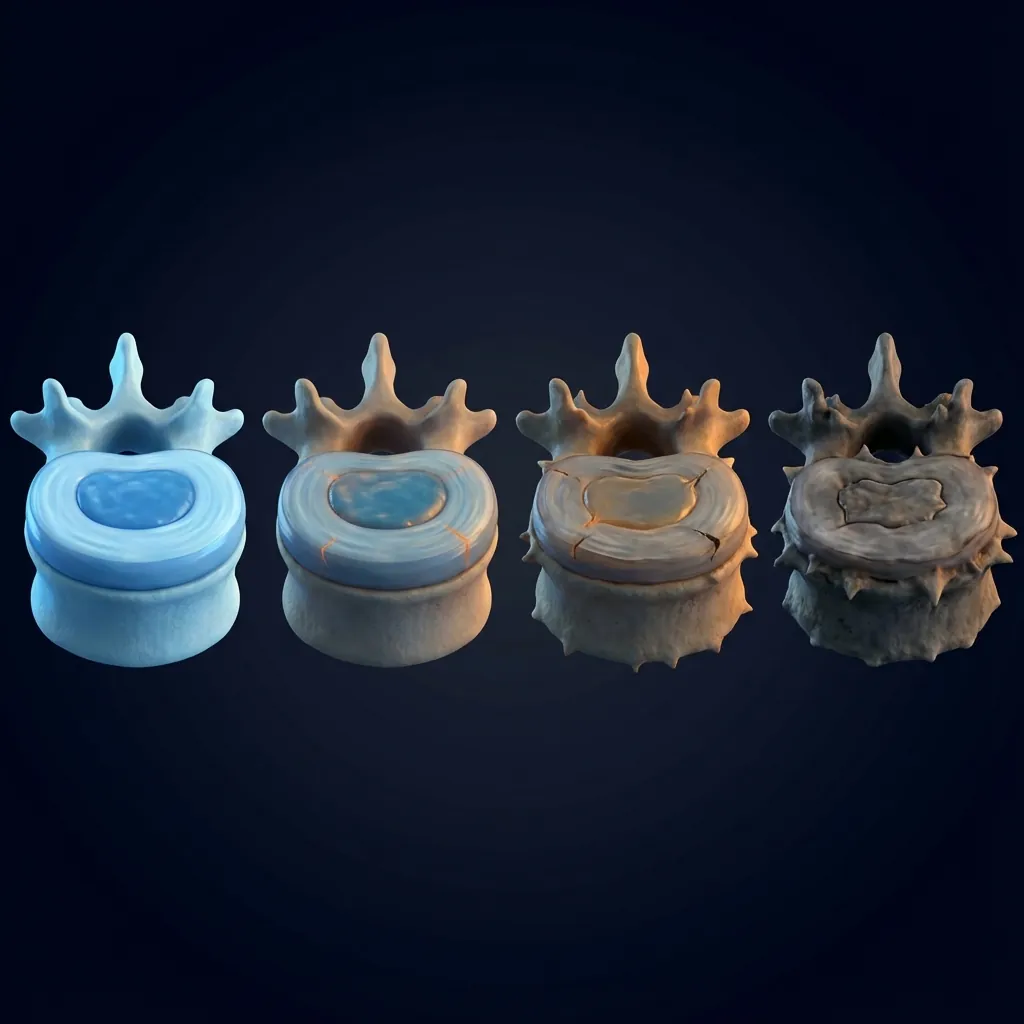
Over decades, repetitive loading from supporting your body weight, combined with bending, lifting, and twisting motions, gradually breaks down the disc material. Micro-tears develop in the annulus fibrosus.
Young discs maintain high water content (70–80%), providing natural cushioning. With age and degeneration, water content decreases progressively to 60% or lower, reducing shock absorption.
The protein matrix (proteoglycans and collagen) undergoes molecular breakdown. Inflammatory mediators accumulate within the disc, accelerating further degeneration.
The annulus develops fissures and tears. The nucleus pulposus may bulge outward or herniate through annular defects. Disc space height gradually narrows.
As the disc space narrows and instability develops, the spine compensates by developing bone spurs (osteophytes) on the vertebral margins, which can narrow nerve passages.
Symptoms Requiring Specialist Evaluation
Not all degenerative findings cause symptoms. Studies show that 40–60% of adults without any lower back pain have significant imaging findings. However, if you experience any of the following, you should seek specialist evaluation:
What Is LumbarDisc Arthroplasty?
Lumbar disc arthroplasty (also called total disc replacement or TDR) is a surgical procedure where the degenerated lumbar intervertebral disc is completely removed and replaced with a sophisticated artificial implant.
Restore Normal Disc Height
Opens the neural foramina, decompresses nerve roots, and restores spinal alignment
Preserve Segmental Motion
Maintains natural flexion, extension, rotation, and lateral bending at that spinal level
Distribute Loading
Shares compressive and shear forces appropriately across vertebral endplates (as a natural disc does)
Maintain Spinal Biomechanics
Prevents the abnormal compensatory loading that develops after fusion

Motion is maintained whilst providing structural support
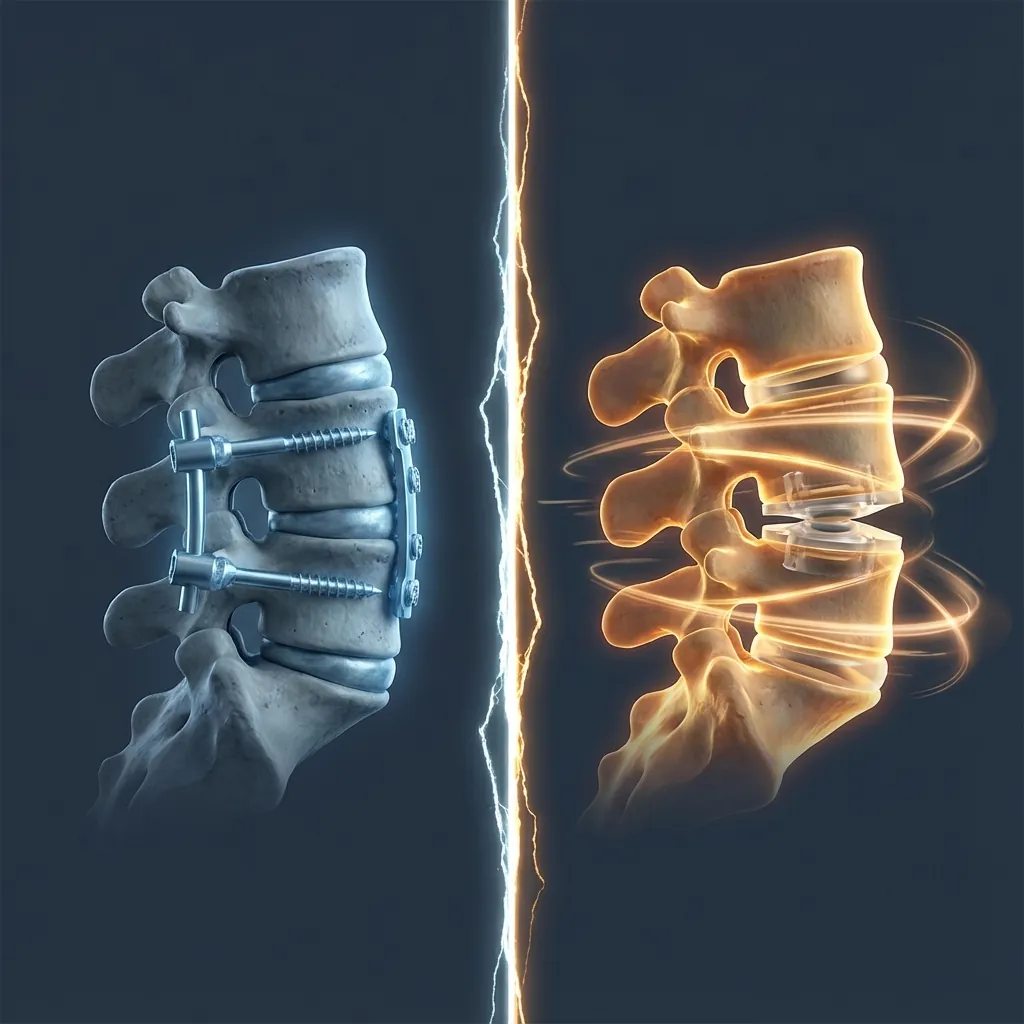
The Fundamental Difference from Fusion
Lumbar Fusion
Permanently joins two vertebrae together using bone graft and/or metal hardware. The fused segment becomes completely immobile—motion is eliminated entirely.
- Loss of motion increases loads on adjacent discs
- Compensatory hypermobility at adjacent segments
- Accelerates degeneration at neighbouring levels
Lumbar Arthroplasty
Rather than eliminating motion, it maintains and restores normal motion using a mechanical device that replicates the natural disc's biomechanical function.
- Preserves spine's natural load distribution
- Significantly reduces adjacent-segment disease risk
- Designed to function reliably beyond 15–20 years
Available Implant Technologies
Ball-and-Socket Designs
Feature a rounded convex surface on one endplate articulating against a concave surface on the other, allowing multi-planar motion. Widely used with extensive long-term outcome data.
Viscoelastic Designs
Incorporate elastic, deformable centres that provide shock absorption and adapt to loading patterns, more closely mimicking a natural disc's behaviour.
Advanced Materials
Modern devices use titanium alloys, cobalt-chrome alloys, and specialised polymers. Many include surface treatments (hydroxyapatite coatings, plasma-sprayed titanium) to enhance biological integration.

Implant selection is individualised based on patient anatomy, bone quality, degenerative pattern, and surgeon preference. Outcome data is generally comparable across different modern device designs.
Why ChooseLumbar Arthroplasty?
The medical literature comparing lumbar disc arthroplasty with fusion demonstrates several consistent and clinically significant advantages for appropriately selected patients.
Adjacent-Segment Protection
50–67% Reduction in Risk
Adjacent-segment disease (ASD) develops in 30–45% of fusion patients within 10 years
Arthroplasty reduces ASD rates to 10–15% at 10 years
2024 systematic review of 2,284 patients confirms significantly lower ASD rates
Protection compounds over decades—potentially preventing one or two future operations
10–15% at 10 years
30–45% at 10 years
10-Year Follow-Up Comparison
| Outcome | Lumbar Arthroplasty | Lumbar Fusion |
|---|---|---|
| Overall Clinical Success | 75–80% | 65–75% |
| Pain Improvement | 50–60% VAS reduction | 45–55% VAS reduction |
| Functional Improvement | 60–75% NDI reduction | 50–65% NDI reduction |
| Patient Satisfaction | 80–90% | 75–85% |
| Adjacent-Segment Surgery | 1–5% | 15–25% |
| All-Cause Reoperation | 7–13% | 15–25% |
| Motion Preserved | 70–85% global ROM | 20–40% global ROM |
CandidacyAssessment
Not everyone is a suitable candidate for lumbar disc arthroplasty. Careful patient selection is essential for achieving optimal outcomes.
Single or Two-Level Degenerative Disc Disease
With clear clinical and imaging correlation (L4–L5, L5–S1, or L3–L4 most common)
Failed Conservative Treatment
Minimum 6–12 weeks of physiotherapy, anti-inflammatory medications, activity modification
Symptomatic Radiculopathy or Discogenic Pain
Documented lower back pain and/or leg pain interfering with work or daily activities
Preserved Disc Height
The degenerated disc retains reasonable height (typically ≥3–4 mm) rather than being completely collapsed
Adequate Bone Quality
Normal bone mineral density (DEXA T-score >–2.0 ideally) to support implant fixation
Healthy Facet Joints
No severe facet joint arthritis (Grade 3–4), which might require fusion instead
Segmental Stability
No significant spondylolisthesis (vertebral slipping >4–5 mm) on flexion-extension imaging
Realistic Expectations
Understanding that surgery relieves pain and restores function but doesn't guarantee perfect outcomes

Medicare and Insurance Coverage (Australian Context)
In Australia, lumbar disc replacement for degenerative disc disease is covered under Medicare item 51130 when performed by an appropriately qualified surgeon.
- Diagnosis of degenerative disc disease with clinical correlation
- Prior failed conservative treatment
- Adequate imaging (MRI, flexion-extension X-rays)
- No severe osteoporosis
Private insurance coverage varies; some policies cover arthroplasty whilst others limit coverage to fusion. Clarify your coverage before proceeding.
Conservative Treatment Requirements
Before considering lumbar arthroplasty, you should have genuinely engaged in appropriate conservative treatment, typically including:
The goal is not indefinite conservative care, but rather ensuring that reasonable, evidence-based non-operative treatment has been given genuine opportunity to help before pursuing surgical intervention.
Surgical Technique& Anterior Approach
Lumbar disc arthroplasty is typically performed via the anterior (front) approach, accessing the spine through a small abdominal incision.
Why the Anterior Approach?
90–120 min
120–180 min
General anaesthesia with endotracheal intubation and muscle relaxation
Step-by-Step Procedure
Recovery Timeline& Expectations
Understanding what to expect during each phase of recovery helps you prepare mentally and practically for your journey back to full activity.
Immediate Postoperative
Days 0–77–9/10 initially; improves by day 3–5
Bed rest first day; encouraged mobilisation from day 1
Incision painful; dressing changed daily
Gentle mobilisation and breathing exercises begin day 1
Strong narcotic pain medications (IV then oral), antibiotics, anti-thrombotics
May be slowed initially; managed with diet and stool softeners
Key Points for This Phase
- Nurses provide wound care
- Physiotherapy encourages gentle mobilisation
- Pain actively managed
Recovery Progress
Phase 1 of 4
What WILL Improve
- Lower back pain typically reduces 50–70% (most patients achieve 70–85% pain reduction)
- Leg pain (radiculopathy) improves 75–90% in most patients
- Functional capacity and disability improve 60–75%
- Ability to walk, sit, stand, and engage in activities significantly improved
- Work capacity restored for most occupations by 3 months
- Quality of life substantially improved by 6 months
Realistic Expectations
- Complete pain elimination is not realistic; mild residual discomfort common (1–2/10)
- Some patients retain mild baseline pain that is much improved but not completely resolved
- Recovery is a gradual process over months, not weeks
- A few preoperative symptoms may persist partially but are usually much improved
- Future pathology at other spinal levels is still possible (though reduced risk with arthroplasty)
Long-Term OutcomesThe Evidence
The most important question patients ask: "Will this work long-term, or will I eventually need more surgery?" Recent prospective studies with very long follow-up provide reassuring answers.

50–60%
VAS Pain Reduction
maintained at 10+ years
60–75%
Oswestry Disability Index
reduction maintained
80–90%
Patient Satisfaction
at 10+ years
70–75%
Work Return
to original employment
Reoperation Rates
7–13%
20–30%
0.7–1.8%
N/A
1.8–5%
15–25%
Motion Preservation
Segmental Motion at Operated Level
Global Lumbar Motion
Progressive Stiffening
Work Capacity
73–74%
13–14%
15–21 Year Long-Term Data
More recent studies extending follow-up to 15–21 years show very long-term durability with no late implant failures, no wear-related deterioration, and no need for implant replacement.
2023 Study Results (20-Year Follow-Up):
Comprehensive Comparison at 10+ Years
| Outcome (Long-Term Follow-Up) | Lumbar Arthroplasty | Lumbar Fusion |
|---|---|---|
| Overall Clinical Success | 75–80% | 65–75% |
| Pain Reduction | 50–70% VAS improvement | 45–60% VAS improvement |
| Functional Improvement | 65–75% ODI reduction | 55–70% ODI reduction |
| Patient Satisfaction | 80–90% | 75–85% |
| Reoperation Rate | 7–13% at 10 years | 20–30% at 10 years |
| Adjacent-Segment Surgery | 1.8–5% | 15–25% |
| Motion Preserved | 70–85% global ROM | 20–40% global ROM |
| Work Return | 73–74% to original job | 60–70% to original job |
| Return to Exercise | Early (8–12 weeks) | Later (12–16 weeks) |
Risks, Safety& Complications
Lumbar disc arthroplasty, when performed by experienced surgeons, is a well-established procedure with a favourable safety profile. Understanding potential complications helps you make an informed decision.
3–5%
Minor Complications
Superficial wound issues, temporary bowel slowing
2–4%
Significant Complications
Requiring additional treatment
<1%
Serious or Permanent
Rare with experienced surgeons
Temporary Complications (Usually Resolve)
Mild Bowel Slowing (Ileus)
5–10%Managed with diet and bowel medications; resolves within days to weeks
Swelling and Bruising
CommonNormal postoperative response; resolves within weeks
Retrograde Ejaculation (Males)
5–10%Semen releases into bladder during ejaculation rather than externally; not dangerous but may affect fertility
Incisional Discomfort
NormalGradually improves during recovery
Temporary Bladder Dysfunction
RareOccurs with prolonged catheter use; resolves after catheter removal
Potential Serious Complications (Rare)
Major Vascular Injury
<0.5%With experienced vascular collaboration
Bowel Injury
<0.5%Infection
<1%Superficial; deep infection rare
Neurological Injury
<1%Deep Vein Thrombosis or Pulmonary Embolism
<1%Prevented with compression stockings, early mobilisation, and sometimes anticoagulation

Factors That Increase Risk
Your complication risk increases if you have any of the following:
Smoking cessation: If you smoke, quitting at least 2–4 weeks before surgery substantially reduces complication risk.
Comparison withLumbar Fusion
Lumbar fusion has excellent short-term and medium-term outcomes and remains appropriate for some patients. However, long-term data show that fusion creates new problems that become increasingly apparent over time.
Why Fusion Has Been Standard
Fusion is particularly useful when:
- Severe segmental instability (spondylolisthesis >5 mm)
- Facet joint arthritis is severe
- Spinal deformity requires correction
- Osteoporosis is significant
The Adjacent-Segment Disease Problem
Biomechanics of fusion complications:
- Fused segment eliminates motion entirely
- Adjacent segments must increase their motion to compensate
- This increased motion accelerates wear on adjacent discs
- Adjacent-segment disease rates climb: 25% at 5 years, 35–40% at 10 years, 45–50% at 15+ years
- "Fusion cascade"—extending the fusion upward or downward to address new adjacent-level disease
Long-Term Satisfaction Comparison
Lumbar Fusion
Excellent initially
Generally maintained
Begins declining
Lower due to secondary procedures
Lumbar Arthroplasty
Excellent initially
Maintained or improves
Remains high
No late decline observed
Common PatientQuestions
Evidence-based answers to the questions patients most frequently ask about lumbar disc arthroplasty.
Modern lumbar disc implants are designed to last for decades. Extensive biomechanical testing ensures they can withstand at least 40–50 million load cycles (representing 40–50 years of normal use).
The lumbar spine, unlike the hip or knee, experiences lower forces and fewer repetitive cycles, so wear is minimal.
Clinical evidence shows no implant failures, no wear-related deterioration, and no need for implant replacement in patients with 15–20+ year follow-up.
Your artificial disc should function reliably for your remaining life.
Lumbar arthroplasty does not prevent future spine problems at other levels. However, because arthroplasty preserves motion and protects biomechanics, you're less likely to need surgery at adjacent levels compared to fusion patients.
If new symptoms develop at a different level:
• You could undergo another arthroplasty at the new level (creating a multi-level motion-preserving reconstruction)
• You could undergo fusion at the new level (hybrid approach)
• Some patients need no surgery and manage conservatively
The key advantage: arthroplasty reduces the likelihood of adjacent-segment disease requiring surgery by 50–67%.
Yes, you can safely undergo MRI imaging.
The titanium and cobalt-chrome implants are non-magnetic and MRI-compatible.
The metallic components may produce some image artifacts in the immediate vicinity of the implant, but this rarely prevents diagnosis.
More distant areas (other spine levels, brain) image normally.
Always inform the MRI facility that you have a lumbar implant so they can adjust protocols accordingly.
Arthroplasty preserves motion, has lower reoperation rates, and better long-term patient satisfaction, but requires more precise surgical technique.
Fusion is more forgiving technically but sacrifices motion and has higher long-term complications from adjacent-segment disease.
For appropriately selected patients (single or two-level degenerative disc disease with adequate bone quality), arthroplasty demonstrates superior long-term outcomes.
Lumbar arthroplasty is generally considered suitable for ages 18–70+, though outcomes are good across ages when other criteria are met.
Younger patients particularly benefit from motion preservation, as they have more years ahead where adjacent-segment disease protection matters.
Older patients can still be excellent candidates if bone quality is adequate and other selection criteria are met.
Age alone is not a contraindication—individual assessment is key.
The implants may trigger metal detectors at airport security, though this is not consistent.
You will be provided with an implant card documenting your surgery that you can show to security personnel.
Modern security scanning technology can usually differentiate between surgical implants and prohibited items.
This is a minor inconvenience that most patients adapt to quickly.
Making YourDecision
Surgery is a significant decision. This framework helps you systematically evaluate whether lumbar disc arthroplasty is right for you.
Self-Assessment Questions
Has conservative treatment been genuinely tried?
Are your symptoms significantly affecting your life?
Do your symptoms correlate with imaging findings?
Are you medically fit for surgery?
Questions to Ask Your Surgeon
About the Procedure
About My Individual Case
About Recovery
Consider a Second Opinion
For any major surgery, consider seeking a second opinion—especially if you're uncertain or have received conflicting advice. A qualified spinal specialist should be willing to discuss your case.
When Arthroplasty May NOT Be Right for You
Reconsider if:
- You haven't tried conservative treatment properly
- Symptoms are mild and manageable with medication
- Imaging doesn't clearly correlate with symptoms
- You have significant anxiety about surgery
Fusion may be better if:
- You have significant spinal instability
- Severe facet joint arthritis is present
- Bone quality is poor (significant osteoporosis)
- More than two levels require treatment
RelatedResources
Explore additional information about spinal arthroplasty and related procedures.
Cervical Disc Replacement
Similar motion-preserving technology for neck (cervical) disc disease
Lumbar Surgical Technique
Detailed technical information about the anterior surgical approach
Radiological Investigations
Understanding the imaging studies used to evaluate your spine
Patient Journey
What to expect from consultation through recovery
Additional Resources
Pre-operative Assessment
Comprehensive evaluation before surgery
Case Studies
Real patient outcomes and experiences
For Referring Doctors
Clinical information for healthcare providers
Note: This information is provided for educational purposes. Always discuss your specific situation with a qualified spinal specialist before making treatment decisions.
Download Your GuidesLumbar Disc Replacement
Free, evidence-based patient guides covering every stage of your lumbar disc replacement journey — from initial assessment through long-term recovery.
Lumbar Disc Replacement Guide
Complete patient guide to lumbar arthroplasty — indications, procedure, recovery, and outcomes.
Pre-Operative Preparation
Everything you need to prepare for your lumbar disc replacement surgery.
Post-Operative Recovery
Recovery milestones, activity restrictions, and return-to-work timelines for lumbar patients.
Exercise & Rehabilitation
Progressive rehabilitation exercises designed specifically for lumbar disc replacement patients.
Medicare & Insurance Guide
Medicare item numbers, health fund rebates, and out-of-pocket cost guidance for lumbar surgery.
Looking for more resources?
Visit the full Patient Resources library for all available guides, including long-term wellness, return to sport, and decision-making frameworks.
Explore Lumbar Disc Replacement In Depth
Continue your research with these focused topics covering every stage of the lumbar disc replacement journey.
Lumbar Spine Anatomy
The five lumbar vertebrae, intervertebral discs, nerve roots, and why lumbar disc degeneration causes back pain and leg symptoms.
Preoperative Assessment
Candidacy criteria, imaging requirements, and the multidisciplinary evaluation process for lumbar disc replacement.
Implant Technology
Lumbar artificial disc designs, material science, biomechanical performance, and 15–20 year durability evidence.
Surgical Technique
The anterior retroperitoneal approach, complete discectomy, endplate preparation, and implant placement for lumbar arthroplasty.
Postoperative Recovery
Recovery timeline, mobilisation protocols, physiotherapy progression, and return to normal activities after lumbar disc replacement.
Long-Term Outcomes & Evidence
Clinical trial data at 5–10 years: pain relief, functional improvement, motion preservation, and adjacent segment protection.
Key Takeaways& Next Steps

Lumbar disc arthroplasty is a proven, evidence-based treatment for carefully selected patients with degenerative disc disease
25+ years of clinical research demonstrates superior long-term outcomes compared to fusion for appropriate candidates
50–67% reduction in adjacent-segment disease preserves your spine's long-term health
80–90% patient satisfaction rates sustained at 10–15+ years follow-up
Motion preservation maintains natural biomechanics and functional capacity
Recovery is typically faster than fusion with earlier return to activities
Your Next Steps
Specialist Consultation
Meet with a qualified spinal specialist to discuss your individual case
Comprehensive Assessment
Undergo imaging and evaluation to determine candidacy
Informed Decision
Review all options and make a decision aligned with your goals
Ready to Discuss Your Options?
Take the first step towards understanding whether lumbar disc arthroplasty is right for you.